Toplines
- Current transparency efforts in health care produce information that’s too complex and hard for consumers to access
- Smartphones, apps, and wearable devices could facilitate a new kind of data transparency that benefits our health
Wednesday, August 23, 2017
By Elena Fagotto and Archon Fung
There are many factors driving the recent push for greater transparency in health care, from the desire to identify waste and reward high-quality, low-cost care to an attempt to close the information gap between patients and physicians.
For more than 15 years the Transparency Policy Project, an interdisciplinary group based at the Harvard Kennedy School, has been studying policies that mandate information disclosure as a tool to curb risks to the public, such as exposure to pollutants, and to improve public services. One of our most important findings is that transparency works only if the pieces of a “demanding action cycle” that translates new information into changes in behavior are in place. The first and most important question for proponents of transparency is: What do you think users will do with the information that you provide?
One problem is that the information produced by transparency efforts may be too complex to understand, so it does not change consumers’ choices. Another is that the information people need may be available somewhere online, but not when and where they make their decisions. For example, information on hospital quality and safety is scattered across different websites, from Medicare.gov to the Leapfrog Group hospital ratings, and even Yelp. Wouldn’t it be easier if patients were offered quality and safety information when they get a referral from their primary care physician or when they book an appointment?
Finally, sometimes information is available, but people don’t use it because they don’t have a choice. People might have data about the health providers in their area, but their options may be confined to health providers within their health plan’s network. Or they may live in areas where only one hospital is available, or they have limited mobility. All of these factors diminish the possibility that people will use information to shop for the best available care.
We also have learned that, when designed correctly and applied to a context where alternatives are easily available, transparency can go a long way. Disclosing restaurant hygiene ratings as simple letters visible to patrons as they walk into a restaurant, for example, created powerful incentives for establishments to become cleaner, and reduced the number of hospitalizations for foodborne illnesses.
With support from The Commonwealth Fund, we are embarking on a project focused on how technological innovations such as smartphones, apps, and wearable devices facilitate a new kind of transparency that might be beneficial for our health. We will begin by interviewing experts to identify the most successful digital platforms through which patients can not only access information, but also generate and share their own health data, and connect with physicians, other patients, and research communities. Platforms in our initial scan include initiatives that connect patients with their peers, such as Smart Patients and MyHealthTeams, as well as patient-powered research networks that allow patients to share their health data to advance medical research.
We will develop detailed case studies to understand these platforms’ common features, the type of data and information that are exchanged, and how such flow of information empowers patients to take better care of their health. We also will examine whether platforms help all patients or only more tech-savvy users. We hope to find new pathways in transparency, especially as we explore how user-generated data feed into health care decisions and how patient communities crowdsource their data to influence medical research.
Article link: http://www.commonwealthfund.org/publications/blog/2017/aug/transparency-and-technology




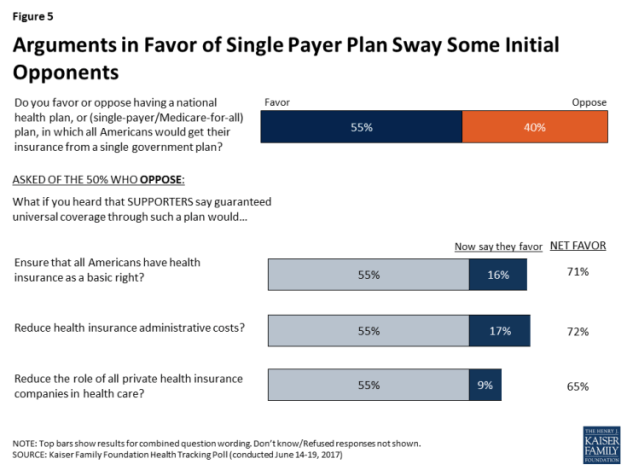 Figure 5: Arguments in Favor of Single Payer Plan Sway Some Initial Opponents
Figure 5: Arguments in Favor of Single Payer Plan Sway Some Initial Opponents
 by
by