Arthur Kellermann April 27, 2017

During Operations Enduring Freedom and Iraqi Freedom (2001–2014), the United States’ military health system completely transformed its approach to casualty care, achieving the highest rate of survival from battlefield wounds in the history of warfare. It is one of the most remarkable accomplishments in the history of US medicine.
Ironically, the same health care system that worked miracles “down range” in Iraq and Afghanistan faces mounting criticism at home. How can this be? In part, it is because the military health system has two distinctive missions: support combat and humanitarian assistance missions overseas and provide comprehensive health services to millions of service members, their families, and military retirees at home.
The core mission of the military health system is unique. Unlike the Department of Veterans Affairs (VA) and large, private health care systems, the military health system must be ready to deploy thousands of health care providers to the other side of the world at a moment’s notice and fly critically wounded warfighters home within one to three days of injury [See Photo Above]. Since the founding of our Republic, military medicine has supported our armed forces whenever and wherever they go in harm’s way.
The other mission of the military health system is to deliver health care at home through a network of military hospitals and clinics, supplemented by health care purchased from thousands of private doctors and other providers. This second mission reinforces the first: Service members stay healthy, and when deployed, they can be confident that their families will be looked after. Military health care providers between deployments maintain their clinical skills by treating service members and millions of beneficiaries. Military hospitals provide valuable platforms for teaching the next generation of uniformed health care professionals and standby capacity for combat casualties.
The Current Challenge
Some critics allege that the military health system’s stateside mission costs too much, delivers care of uneven quality, and doesn’t attract enough complex cases to keep provider skills sharp between deployments. They want the Department of Defense to close most of its remaining facilities, outsource the care to the private sector, and position more military providers in civilian hospitals. Before these ideas receive serious thought, it is worth examining the assumptions on which they are based:
Costs
According to the Congressional Budget Office (CBO), the Department of Defense spends $52 billion, about 10 percent of its budget, to provide a variety of services to 9.4 million beneficiaries. This total includes costs not counted by civilian health systems, such as $1 billion annually for military health research and billions more for “TRICARE for Life,” a first-dollar, wraparound plan Congress mandated to supplement the Medicare coverage of military retirees. In fact, yearly spending varies by $2 billion or more due to fluctuations in military construction. To put this in context, in 2016 Kaiser Permanente collected $64.6 billion to care for its 11.3 million members. The Department of Defense’s FY2017 budget for military health is $48.8 billion to care for its 9.4 million beneficiaries.
Growth in health care spending is not limited to the military. Civilian health spending has outpaced our nation’s economy as far back as 1950. Between 1999 and 2009 alone, health spending grew so fast, it wiped out the income gains of average US families. Military health spending grew too, but recently it has increased at a far slower pace than civilian health spending. According to the Centers for Medicare and Medicaid Services (CMS), between 2009 and 2015, civilian health spending increased 32.6 percent. During the same timeframe, military health spending grew 13.9 percent (See Exhibit 1). A recent analysis produced by the CBO attributes most military health spending growth since 2000 to congressionally mandated expansion of TRICARE benefits, including the establishment of TRICARE for Life, an insurance option that eliminates most out-of-pocket costs faced by Medicare-eligible military retirees and their families.
US health care is not only costly; it is inefficient. The National Academy of Medicine estimates that our nation wastes $750 billion per year on “unnecessary or inefficient services, excessive administrative costs, high prices, healthcare fraud and missed opportunities for prevention.” In 2015, aggregate health care spending approached $3.2 trillion dollars. Only 1.5 percent is devoted to military health. Given these facts, it is hard to see how outsourcing more care will save money.
Quality
Critics assert that the military health system does not perform enough complex surgical procedures in peacetime to maintain provider skills. The volume-quality relationship is strong, but it is not absolute. High-quality training and strict adherence to procedures—an approach first championed by military aviation—can largely compensate for smaller case volumes. In 2014, the military health system compared its performance to three of our nation’s top health care systems—Geisinger, Intermountain Healthcare, and Kaiser Permanente—and found that it did better in some areas, worse in others, and generally as well overall.
A recent American College of Surgeons assessment of surgical outcomes, based on national data, identified several military health system hospitals as top performers. Another study found that the military health system does not have the racial disparities in care commonly seen in civilian hospitals. A recently published analysis of more than 10,000 military health system beneficiaries with carotid artery stenosis (a condition that can lead to stroke) found that patients treated by military doctors got fewer procedures but had better outcomes than beneficiaries treated by private, fee-for-service doctors.
Productivity
Is the military health system less productive? That depends on how productivity is defined. Because most civilian hospitals rely on fee-for-service billing, their staffs have a strong incentive to see lots of patients and order large numbers of tests and treatments. This translates into the appearance of productivity as measured by “relative value units” (RVUs)—the most commonly used metric of clinical workload. There are two problems with this approach, however. First, RVUs measure the volume of care, not its value. It doesn’t even matter if a procedure helped the patient; it only matters that it was done. Second, RVUs undervalue primary care and overvalue procedures performed by specialty providers. As a result, keeping patients healthy looks less “productive” than filling hospital beds and performing lots of complex procedures.
Consider the previously-mentioned study of military health system beneficiaries with carotid artery stenosis. Although military doctors performed fewer expensive procedures and the patients they treated were less likely to die or have a stroke than those treated by fee-for-service doctors, judicious management looks less “productive” since it generates fewer RVUs.
The purpose of the military health system is to protect the health of the force, not to generate RVUs. In 1866, Dr. Jonathan Letterman, the “father of battlefield medicine,” wrote: “A corps of medical officers was not established solely for the purpose of attending the wounded and sick. The leading idea is to strengthen the hands of the Commanding General by keeping his army in the most vigorous health, thus rendering it, in the highest degree, efficient for enduring fatigue and privation, and for fighting.” In light of this responsibility, using RVUs to assess the clinical productivity of the military health system makes as much sense judging the effectiveness of a combat unit by counting the number of bullets it shoots.
Finding A Better Way
Rather than dismantle the military health system, policy makers should let it operate more efficiently. Among the options that follow are four opportunities created by provisions embedded in Section VII of the 2017 National Defense Authorization Act (NDAA):
- Make greater use of enlisted providers—Overseas and aboard ships, the military health system relies on its corpsmen, medics, and med techs to deliver routine care under supervision, as well as save lives in combat. However, the moment these skilled providers come home, they are relegated to minor clinical or clerical tasks because no comparable role exists in civilian health systems. If the military health system allowed them to function as “primary care technicians,” it could expand access to care, reduce use of emergency departments and urgent care centers, and strengthen readiness for future deployments.
- Consolidate treatment of complex cases—When a service member is wounded in combat, he or she is MEDEVACed to the nearest combat support hospital, then flown by Critical Care Air Transport to a stateside military hospital. Two decades ago, the military health system used a similar approach inside the United States to concentrate complex care to its top medical centers. If it reinstituted the practice, patients and taxpayers would benefit. Studies show that Walter Reed’s Murtha Cancer Center achieves better outcomes at lower cost than comparable civilian cancer centers.
- Systematically improve practice—Many of the advances in trauma care in Iraq and Afghanistan came from the Joint Trauma System, which systematically analyzed casualty data to identify opportunities to improve. If the military health system employed a similar approach to assess delivery of high-risk care in stateside hospitals, it could ensure that beneficiaries get the right care at the right place for the right reason.
- Standardize to optimize—The US armed forces have learned the value of training and fighting as a joint force. Military health care providers have learned the same lesson in combat zones but when they return home, they tend to revert to the old ways. Some variations in approach are inevitable, but the military health system should strive to standardize key workflows, equipment, and even the layout of its operating rooms and delivery suites. That way, when a military health system provider rotates to a new hospital, he or she can swiftly integrate into a new health care team.
- Keep patients healthy—In war zones, protecting the health of the force is a top priority. Taking an equally diligent approach to population health at home could produce substantial benefits. Redoubling efforts to boost rates of vaccination, discourage smoking and use of smokeless tobacco, prevent injuries, and treat hypertension and obesity could generate huge downstream savings.
- Treat selected civilians—In war zones, commanders have the latitude to treat ill and injured civilians if doing so will help win the support of the local population. Currently, most lack this authority in the United States. At present, only two military medical centers participate in their state’s trauma system. If more were allowed to do so, their medical staffs would benefit from the extra caseload, and the civilians they treat would benefit from the world-class trauma, burn, and rehab care available at these medical centers. Any VA hospital with a waiting list should preferentially refer its patients to the closest military hospital. Section 717 of the NDAA should facilitate the needed changes in policy.
- Ensure clinical proficiency—Military surgeons are already partnering with the American College of Surgeons to devise objective ways to assess surgeons’ readiness to deploy. Recently, they devised a way to cross-walk Current Procedural Terminology codes used to track performance of surgical procedures to critical wartime surgical skills. Once this approach is refined, it will be extended to other wartime specialties such as emergency medicine, anesthesiology, and intensive care. This will help the military health system comply with Section 708 of the NDAA.
- Measure what matters—To ensure military providers address the “quadruple aim”—readiness, better health, better care, and lower per capita costs—the military health system has adopted 30 “Partnership for Improvement” measures. Adopting a smaller, high-yield set of “vital signs” metrics devised by the National Academy of Medicine would allow military health system leaders to compare their system’s overall performance to other large health systems and satisfy Section 730 of the NDAA.
- Embrace Telehealth—In deployed settings, the military health system uses telehealth to support health care providers working in small forward operating bases and on ships at sea. Global teleconferencing allows trauma experts across 12 time zones to regularly meet, discuss complex cases, and identify opportunities to improve. Despite its success with telehealth overseas, the military health system was slow to adopt it at home due to stringent information security requirements and budgetary constraints. Section 718 of the NDAA directs the military health system to rapidly expand the use of telehealth in its clinical operations.
- Centralize licensure and credentialing—Typically, military health care professionals change duty stations every two or three years. Federal law allows those licensed in one state to practice in others, but only on federal property. If providers could reach outside their treatment facilities, the military health system could fully use telehealth and improve access to care. Provider credentialing is equally cumbersome. Although the military health system has a global reach, it still credentials most providers at the facility level. A systemwide approach makes more sense.
Facing the Future
In Iraq and Afghanistan, the military health system demonstrated a remarkable capacity to innovate when necessary to protect the health of US and coalition forces. Dr. Don Berwick, founder of the Institute for Healthcare Improvement, recently observed that “Military medicine put the learning health system framework into practice before the Institute of Medicine described it.” Today, US soldiers, sailors, airmen, and Marines know that if they are badly wounded in combat, the military health system offers their best chance of coming home alive and recovering. This confidence is a force multiplier on the battlefield.
Looking forward, we cannot assume that future conflicts will resemble the most recent ones. As US forces evolve to meet the threats posed by near-peer adversaries, the military health system must evolve, too. The best way it can maintain readiness to support combat operations and strengthen its capacity to innovate is to employ the same techniques, teamwork, and enterprising spirit that serve it so well “down range” to meet the health care needs of its beneficiaries in the United States.
Coaches often remind their teams that “You play the way you practice.” By “practicing” at home the way it “plays” overseas, the military health system can deliver better care at lower cost and strengthen its capacity to support and sustain our armed forces on any future battlefield.
Exhibit 1: Military Health Spending, 2006–2015
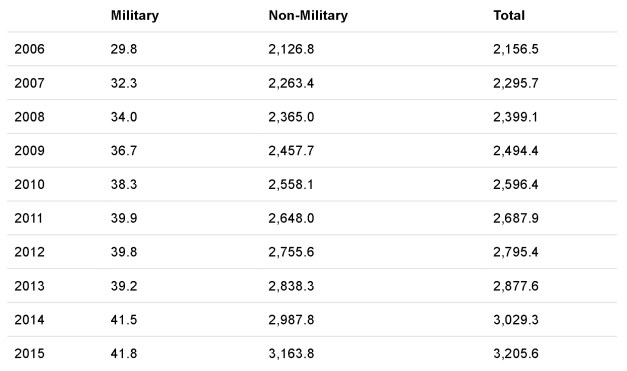
Source: National Health Expenditure 2015 Centers for Medicare & Medicaid Services, Office of the Actuary, National Health Statistics Group from the methodology paper. Note: Department of Defense spending for health care services (hospital, ambulatory care, provider, diagnostics, pharmacy, etc.) an this total does not include the cost of accrual payments made to fund TRICARE for Life. Non-Military: Includes out of pocket, private insurance, Medicare, Medicaid, CHIP, VA, Worker’s compensation, Indian Health Services, General Assistance, Vocational Rehabilitation, maternal/child health, other federal and state programs that provide subsidies, high risk pools under ACA, school health, public health, SAMHSA treatment services, investments in research and facilities. Total spending for health care, including federal and state programs, private health insurance, and out-of-pocket spending. Column numbers may not add to totals due to rounding. Dollar amounts shown are in current US dollars.
Author’s Note
The author is dean of the School of Medicine at the Uniformed Services University (USU) of the Health Sciences, and as such he is an employee of the Department of Defense. His views are his own and do not necessarily reflect those of USU, the military health system, the Department of Defense, or the US government.
Article link: https://www.healthaffairs.org/do/10.1377/hblog20170427.059833/full/


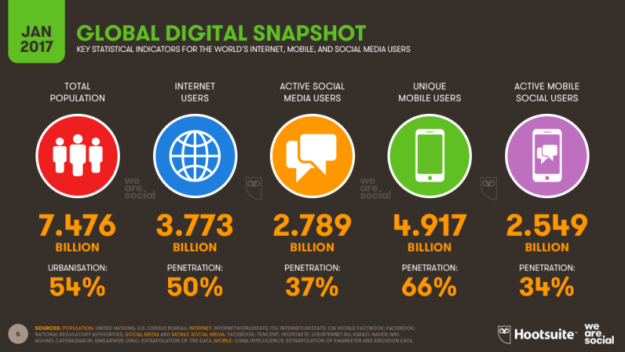
 Over 16 million text messages are sent in one internet minute in 2017.
Over 16 million text messages are sent in one internet minute in 2017.






 Since 2001, the Department of Veterans Affairs (VA) has tried three different modernization programs for its healthcare system. So when the department announced another plan to modernize by adopting the same system as the Department of Defense (DoD), the Subcommittee on Information Technology was skeptical and interrogated them in a
Since 2001, the Department of Veterans Affairs (VA) has tried three different modernization programs for its healthcare system. So when the department announced another plan to modernize by adopting the same system as the Department of Defense (DoD), the Subcommittee on Information Technology was skeptical and interrogated them in a 