Various governments around the world are planning to use Blockchain or distributed ledger technology (DLT) in their bid to establish a national identity system in their jurisdictions as of early October 2017. These systems are intended to be safe and secure and can be used in both public and private transactions.
The need to create said systems is driven by the susceptibility of existing systems against various risks like identity theft. An example is the case of consumer credit reporting agency Equifax, whose latest data breach has resulted in the theft of personal data of over 140 million individuals.
Countries and states using DLT to establish national identity systems
Several countries are piloting the use of DLT to create their own national identity systems that span the private and government sector. Among these countries is Singapore, which is eyeing a system that would expand beyond the functions of its existing citizen account for e-government services called the SingPass. The initiative is part of the Singaporean government’s smart nation program.
Estonia, meanwhile, is another country which successfully utilized DLT to create its identity system called ID-kaarts. Among the benefits of the system are an all-digital government experience enjoyed by all citizens, substantial reduction of bureaucracy, and high citizen satisfaction with their government transactions.
Moreover, the state of Illinois has launched a pilot trial on a Blockchain-based birth registry/ID system with a goal to individualize and secure identities. The state government is partnering with Utah-based company Evernym and is expected to use the Sovrin Foundation’s publicly accessible distributed identity ledger in the project.
Benefits of DLT-based identity systems
There are several expected benefits of using DLT in creating identity systems. Among these are the shift of power and profit from data management to individual owners from major companies and the right of the owner to “sell” his/her own data.
With the increasing fear of voting fraud, Blockchain projects can now secure a digital ballot box or voting system based on Blockchain to prevent voter fraud during elections. Once cast, votes would be unalterable results and available for everyone to see.
Under a Blockchain system, voters are able to cast their votes from their mobile phones or personal computers, which are then logged into an immutable Blockchain and utilized to reliably verify the results of the election.
According to Jamie Skella, co-founder of Horizon State, one of the companies that builds such systems, there is a need for better decision-making tools and processes to achieve the best outcomes in a democratic form of government.
“Democracy is the opportunity to share in the decision-making processes that relates to the shared matters which affect us. Democracy is about reaching consensus on how to best use our shared resources to achieve the best outcomes for our partners, children, colleagues, staff, and fellow citizens. Where there are shared resources in any cooperative environment, there remains no question: we need better shared decision making tools and processes.”
How Blockchain is changing elections in the 21st century
Blockchain technology is revolutionizing the global political landscape toward direct democracy, where voters can decide the course of government policy themselves.
A digital ballot box represents a smart and cost-effective solution to effectively improve the existing voting procedures. This system will eliminate such issues as manipulation, recording errors, and tampering, as well as encourage voters’ participation.
Although Blockchain-based voting solutions are still in their infancy, they are already showing many and diverse use cases. Governments’ ability to engage and manage a constituency is vital to the future of society, therefore, they should promote and adopt Blockchain to become a key part of the voting process.
Achieving an interoperable health care system remains a top US policy priority. Despite substantial efforts to encourage interoperability, the first set of national data in 2014 suggested that hospitals’ engagement levels were low. With 2015 data now available, we examined the first national trends in engagement in four domains of interoperability: finding, sending, receiving, and integrating electronic patient information from outside providers. We found small gains, with 29.7 percent of hospitals engaging in all four domains in 2015 compared to 24.5 percent in 2014. The two domains with the most progress were sending (with an increase of 8.1 percentage points) and receiving (an increase of 8.4 percentage points) information, while there was no change in integrating systems. Hospitals’ use for patient care of data from outside providers was low, with only 18.7 percent of hospitals reporting that they “often” used these data. Our results reveal that hospitals’ progress toward interoperability is slow and that progress is focused on moving information between hospitals, not on ensuring usability of information in clinical decisions.
1A Jay Holmgren (aholmgren@hbs.edu) is a doctoral student in Health Policy (Management) at Harvard Business School, in Boston, Massachusetts.
2Vaishali Patel is a senior advisor in the Office of Planning, Evaluation, and Analysis, Office of the National Coordinator for Health Information Technology, Department of Health and Human Services, in Washington, D.C.
3Julia Adler-Milstein is an associate professor of medicine in the School of Medicine, University of California, San Francisco.
By ANAHAD O’CONNOR Jody Christ, in her home in Elysburg, Pa., says genetic testing saved her life, though experts warn such tests require caution.Credit Mark Makela for The New York Times
For years, Jody Christ, 62, struggled to control her high cholesterol. Her doctors encouraged her to exercise, change her diet and lose weight, but none of that ever seemed to lower her numbers.
When her health plan, the Geisinger Health System of Pennsylvania, offered a genetic test that screens for dozens of hereditary diseases, she submitted a saliva sample and awaited the results. The test revealed she had familial hypercholesterolemia, an inherited condition that causes the body to churn out cholesterol. Her doctors followed up with additional medical tests that showed Ms. Christ had life-threatening blockages in three coronary arteries, prompting triple bypass surgery last year. They also tested her daughter and granddaughter and found that they, too, had the condition, which affects an estimated one million Americans.
Ms. Christ, who lives in Elysburg, Pa., has since gotten her cholesterol under control with medication and credits the genetic test with saving her life. “If I had not taken that test I might be dead by now,” she said.
Geisinger’s genetic screening panel is currently available only to patients in its health system. But the organization has partnered with a Silicon Valley start-up called Helix, one of a growing number of digital health companies — perhaps the best known is 23andMe — in an effort to make its genetic services more widely available to the public.
Experts say many people are using a growing stream of genetic data to help them make better health decisions. But they also warn that some consumers may be led astray by genetic findings that are overblown or irrelevant. The Centers for Disease Control and Prevention, for example, takes a cautious approach to personal genomics tests, telling consumers on its website to “think before they spit” and that “evidence on the ability of genetic information to change health behavior has been lacking.”
For an initial fee of $80, customers send a sample of their saliva to Helix, which sequences a small chunk of their genome called the exome — the part that houses most disease-causing mutations — and stores the genetic data. Customers can then go to the online Helix store — something like Apple’s app store — and pay its partner companies to comb through their data in search of genes linked to diseases, traits or health conditions.
So far some two dozen companies have partnered with Helix. One is Sema4, which was spun out of the Mount Sinai Health System and sells a test on the Helix platform that determines whether people are “carriers” of genetic variants linked to 67 hereditary disorders, including cystic fibrosis, sickle cell anemia and Tay-Sachs disease. The service, called CarrierCheck, costs $199 and is marketed toward couples who want to know the likelihood of their children inheriting a severe disease.
Another company, Invitae, plans to offer two separate screening panels to Helix customers. One looks for genetic variants linked to breast, ovarian and colon cancer. Another, expected to be introduced later this year, will look for hereditary heart conditions such as cardiomyopathy and various arrhythmias, potentially in people who have no idea they’re affected. “This is really for people who don’t have any reason to think that they’re at particular risk — but the problem is you really don’t know unless you do the genetic test,” said Dr. Robert L. Nussbaum, Invitae’s chief medical officer.
Other companies that partnered with Helix include EverlyWell, which analyzes genes linked to metabolism, and Admera Health, which predicts how people will respond to medications based on their genetic profiles. Additional services claim they can tell from your genes and other information how you’ll respond to exercise, which foods you should eat, and even which types of wine you might prefer.
Dr. Eric Topol, a cardiologist and professor of genomics at the Scripps Research Institute in California, said there was great potential value in consumer genomics tests, particularly with services like those developed by Geisinger, Invitae and Sema4 that are backed by strong data. But he cautioned that there was not enough evidence for many of the genetic claims being made about exercise and nutrition, and worried that many people would not be able to distinguish the services that are scientifically rigorous from those that are not.
“There’s this mixture of some that have real solid footing and then some that have zero footing,” Dr. Topol said.
Joel C. Eissenberg, a professor and associate dean in the department of biochemistry and molecular biology at the Saint Louis University School of Medicine, said that unlike some direct-to-consumer tests, like whole-body CT scans, which can expose consumers to potentially harmful radiation, personal genetic tests pose no risk of physical harm. “I’m a big fan of the democratization of health care delivery, wherever it’s not a risk for the patient,” he said.
A negative side effect from genomics testing is distress when people discover they have a mutation linked to a disease, studies have shown, though the anxiety tends to be short-lasting. In April, 23andMe received approval from the Food and Drug Administration to market the first direct-to-consumer genetic tests for 10 diseases, including Alzheimer’s and Parkinson’s, with no doctor involved. The company, however, does offer links to genetic counselors on its website for those who desire follow-up.
Unlike 23andMe, most companies require some sort of approval from a doctor for personal genetic tests. When customers order a test from Sema4 through Helix, for example, a physician “reviews their report, signs off on it, and then you’re genetically counseled around that report,” said Eric Schadt, the company’s chief executive.
Invitae has a similar protocol in place for its cardiac disease test. Customers will have to fill out a health questionnaire, and those with a strong family history of heart disease will be referred to a doctor for more in-depth diagnostic testing.
“You have to have a physician involved in ordering this test,” said Dr. Nussbaum, Invitae’s chief medical officer. “But it’s really designed for the motivated and educated consumer to initiate the process.”.
U.S. hospitals and health care groups have experimented over the past decade with new management structures and alternative payment models to provide quality health care at lower cost. But physicians have been slow to embrace these for a host of reasons. Chief among them, our research shows, is that they feel excluded from the process.
The only practical way to make value-based care a reality is for health care organizations to bring physicians back into the decision-making process. After years of experimentation, doctors want evidence that new models for health care management, reimbursement, and policy will actually improve clinical outcomes for their patients. Without it, they see little reason to alter the status quo. That’s a fundamental and overlooked obstacle to progress. And it explains why management-led organizations that have not embraced physician input have run into resistance.
It may sound odd to suggest that the industry overlooked physicians as it set about reshaping the health care system. But that’s how physicians see it. With our colleagues at Bain & Company, we recently surveyed 980 U.S. physicians in eight specialties, 100 health system finance officers, as well as 100 health system procurement officers — the people in charge of buying supplies for hospitals. What we found was startling: Physicians clearly understand the challenge posed by rising costs for clinical care and prescription drugs, but many don’t feel they are in a position to help rein in costs. They do not feel sufficiently engaged in making important decisions about cost control, performance improvement, and adoption of new reimbursement models. Indeed, many feel overruled, with mandate after mandate from hospitals and management-led health organizations being done to them, not with them.
How leading providers are delivering value for patients.
By sidelining doctors, the health care industry has overlooked a key principle in change management — and undercut its own efforts. Physicians who are not aligned and engaged with their organization have more reasons to resist new systems, such as value-based-payment models. By contrast, physicians who are engaged in decision-making are much more satisfied with the working environment and are more willing to lead change. Our research and experience shows that health care organizations that give physicians a say in management decisions are able to create greater momentum for change.
Physicians are particularly hesitant to embrace new systems when the clinical implications and the return on investment are unproven and the administrative burden is significant. A comparison of our 2015 and 2017 survey findings shows a notable slowdown in the adoption of value-based payment models. Two years ago, many physicians expected a broad rollout of value-based care and a corresponding decline in practices exclusively using the traditional fee-for-service model. But providers have been slow to embrace value-based care, citing concerns about implementation and lack of evidence that it results in better outcomes.
More than 70% of physicians told us they prefer the fee-for-service model, citing concerns about the complexity and quality of care associated with value-based-payment models. Fifty-three percent of physicians say that capitation reduces the quality of care, and most see little advantage from pay-for-performance models either. Further, many believe their organizations are not sufficiently prepared for the shift to value-based care.
One bright spot is the evolving role of physicians in the purchase of medical equipment. It highlights the kind of collaborative approach to decision making that could help create a more supportive climate for value-based care. Ten years ago, hospitals shifted decision making away from surgeons and toward procurement professionals who chose products mainly on the basis of price, often putting the two groups at odds. Since then, many hospitals in the United States have reversed course, giving surgeons a bigger say in medical-equipment purchasing — and that’s transformed attitudes. More than 80% of surgeons and procurement officers told us they now work in collaborative partnerships to purchase medical equipment, weighing clinical and economic value together, and surgeons broadly support this arrangement
Collaboration has created a virtuous circle. As surgeons take on greater decision-making authority, they become more sophisticated buyers, weighing both clinical and financial data when they select devices. Forty-three percent of surgeons now believe their procurement department improves costs and quality of care. Surgeons engaged in decision making also are more likely to promote their organizations and be aligned with their missions.
Giving physicians a greater say increases their commitment to change. When we asked physicians if they would recommend their organization as a place to work and practice, we found a 108-point difference (+47% vs. -61%) between those who said they were highly engaged in decision making and those who were not.
Health care organizations can generate greater support for value-based care by working closely with their physicians to shape these models and addressing doctors’ concerns about implementation and outcomes. It will take time to develop clinical and economic evidence, which means the pace of change will remain slow. But it will also help the industry move toward better solutions.
by Brian Behlendorf, executive director, Hyperledger
It would be diplomatic to say that the rise of open standards and APIs in the healthcare industry has yet to truly pay off in the form of better widespread patient data portability, reduced complexity in the systems behind payments and claims, better quality metrics and outcomes, or better automation of menial paperwork or other manual process. Our health IT systems are only getting more and more silo-ed and disintegrated, and there’s always a new venture-backed SaaS provider or software vendor who just wants to solve that by centralizing (er, “vertically integrating”) all data and processes on their systems, adding to the problem rather than solving it. The client-server model for applications just doesn’t work for an industry as complex, heterogenous, and political as healthcare. Could blockchain technology be helpful here?
Blockchain technology first rose to prominence as the data and networking architecture underpinning cryptocurrencies like Bitcoin. We believe the decentralized ledger and smart contract features will have the most significant impact on society. A blockchain can reinvent any multi-party system of record from one that depends on a central trusted third party to maintain integrity and trust, into a decentralized, distributed, and auditable networked database. Pilot projects are underway in financial markets settlement, supply chain tracing, intellectual property and even property title. Increasingly, the healthcare sector is looking at blockchain too.
So, what’s a blockchain, really?
Let’s start with the basics. A blockchain is a stream of data – a distributed ledger – that is written to, shared with and confirmed by a collection of nodes on a common network, run by different companies or organizations. The software used to build a chain ensures that everyone on the network sees, validates, and confirms each proposed next “block” of data in the chain, with links to the prior and/or next block in the “chain”.
This blockchain validation step is the key that allows a blockchain to replace a trusted intermediary. For example, if any node on the network tries to transfer a particular asset twice, to two different parties, that transaction would not be validated by others on the network, and there would be no agreement to add it as a new block on the chain. This validation, this immediate confirmation from the whole of the network, and this distributed-at-all-times nature of the chain is what builds trust in the system as a whole – the same rules apply to everyone, and we don’t need to depend upon just one party to set those rules and keep the ledger consistent and honest.
Also important here are “smart contracts” on a ledger – these are simple software programs that run across all nodes in the network, and can extend the validation logic at each node, in a way that is automatable and undeniable. In the financial world, an example might be an insurance contract, or an offer to buy a share of stock in the future for a certain price set today. In a healthcare setting, where a chain is being used to share personal data, this can be used to implement an authorization process and confirmation step that notifies the patient – or even put them in control – when their data is shared from one address to another.
Confidentiality and privacy on a chain
Since all data is copied to every entity on the chain, confidentiality and privacy need to be carefully designed in. Furthermore, this widespread distribution means space is at a premium, so small data or metadata is preferred. That means the way you design your blockchain application is important – what you decide to store “on-chain,” so you can get it everywhere and with high integrity, versus what you store “off-chain” because of size constraints or confidentiality, is key. In healthcare we sometimes deal with very large files (such as X-ray scans) – there’s no need to store those entirely on the chain, but storing links to those as well as a “hash” to ensure that it hasn’t been changed, would likely be right.
Not all ledgers are publicly available. Just as you might have a private network at your house, or use a VPN to connect to the office, there will be private or “consortium” chains running between specific organizations, perhaps with a legal or regulatory agreement binding the participants. For example, a healthcare data chain may limit its network nodes to only HIPAA-covered entities, in addition to encrypting some data and leaving other data “off-chain”, so as to provide multiple layers of security.
Which solution/improvement has the most potential to drive blockchain adoption across the healthcare industry?
Current blockchain healthcare efforts include:
Blockchain Health is implementing permissions management for data from clinical trial patients, easing the burden for recording agreements and demonstrating audit compliance.
More efficient billing and payment – benefits being automation, transparency, better records management. Could lead towards better outcomes-based payments.
Provenance tracking of pharmaceuticals, from manufacturing (anti-fraud, public health) all the way to consumer adherence (imagine smart pill bottles that help the elderly and caregivers with dosages).
Blockchain technologies hold the promise to unite the disparate processes in healthcare, increase data flow and liquidity, reduce costs and improve patient experience and outcomes. Blockchains depend upon ecosystems of peers participating in a network, and are designed to avoid the need for any to have to be the gateway at the center. The health information industry must start thinking and planning for chains, building proofs of concept, running pilots, and organizing itself to take advantage.
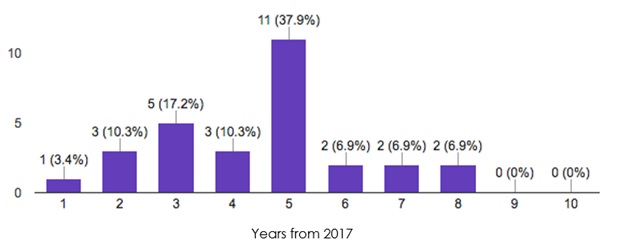
How long before [healthcare] first adopters utilize blockchain in large scale solutions?
How long before blockchain solutions realize mainstream adoption?
Source: January 2017 Hyperledger Healthcare Working Group Survey, N=29
Like we saw with the HIE debate, there will be a natural tendency to build small, regional or use-case-specific chains; this would be a mistake, as the more participants and nodes on a chain, the greater the overall utility for the patients and greater economic value you can create for other participants.
Hyperledger is committed to helping the healthcare industry realize the full potential of open source blockchain technologies. So, as this industry investigates this space, we should focus on pilots, but also, on how to quickly grow them into full-fledged production systems for a large number of participating organizations. We hope to see you out there!
DoD should join other logistics-heavy organizations in experimenting with the cryptography-messaging-accounting technology that powers Bitcoin.
It’s no surprise that the Defense Department faces challenges in managing its inventory, whose value is ballparked at nearly $100 billion. It is difficult, not to mention costly, to manage and track the purchasing of hundreds of thousands of parts from a global web of sub-suppliers, many of them small, unsophisticated, and several steps removed from whatever complicated product the Pentagon is buying.
A 2015 report by the Government Accountability Office, for example, reported “weaknesses in the management of its supply chain,” including problems tracking and delivering supplies. And it’s one thing to misplace materiel, but troops and even missions can be put at risk when shoddy subcomponents enter the system. Over the past seven years, Congress and DOD have ratcheted up their attention to the problem of counterfeit parts, particularly after some sensitive and costly fixes to semiconductors, missile defense systems, and fighter jets. Industry sat up and took note, and Congress required more reporting of counterfeit parts, but problems continue.
But a new technology being tested by other logistics-heavy organizations may offer some help.
Most people, if they’ve heard “blockchain” at all, probably associate it with Bitcoin, Ethereum, or other cryptocurrencies. But it is more precisely the technology that underlies those products. A combination of cryptography, distributed messaging, and other technologies, it is at heart an accounting system with a transparent, ultrareliable mechanism for validating transactions.
This makes blockchain very attractive to companies that depend on the purchase and distribution of vast amounts of material from many sources to many places. Already, major industry players in agriculture, shipping, and retail are putting it to use. For instance, IBM is working with Walmart and China’s Tsinghua University to use blockchain technology to digitally track movement of food products. According to IBM, “farm origination details, batch numbers, factory and processing data, expiration dates, storage temperatures and shipping detail are digitally connected to food items and the information is entered into the blockchain along every step of the process.” Every participant can verify each of the data points through a digital consensus system, leading to an unalterable record of the transaction.
Similarly, shipping giant Maersk is working with Microsoft and consultants EY on a blockchain pilot to track shipments in real time, lower the costs of insuring international maritime shipments and increase the assurance of all parties to the transaction. Even the United Nations is using blockchain to process assistance, support digital identity, and manage contracts when traditional methods are unavailable or fall prey to vulnerabilities.
Blockchain solves a number of challenges. Control or verification is executed by consensus, rather than a central body, limiting the security problems of a single point of failure or vulnerability. Each step in a transaction is tracked, so if a problem occurs with a shipment, the recall of similarly manufactured products can be tracked to a more specific vulnerability point and not require an overly broad and expensive recall. The incremental costs of verification are modest, and the ledger is visible to all participants, allowing even small suppliers to participate and carry out best practices. And the transparent nature of the ledger cuts down on—if not eliminates altogether—corrupt practices that can undermine licensing and customs regimes.
Blockchain can even help with problems specific to government and the Defense Department. Small companies are often not in a position to finance and manage the tracking, auditing, and oversight mechanisms necessary to comply with government, particularly defense, protocols. Yet DOD’s supply chain depends on an enormous number of globally distributed companies, making it hard to oversee them all. This has traditionally been part of the challenge of developing anti-counterfeit systems. Blockchain may offer a simpler way to comply, broadening the set of companies that can compete for military contracts without watering down oversight.
Granted, there are special considerations that other industries simply don’t have to address, such as DoD’s need to maintain extra security and its reluctance to allow non-U.S. access to even hosting its cloud storage. But there are ways to soothe these concerns. For example, the military might create a private blockchain, accessible by invitation only. Or a hybrid ledger, with some transactions highly permissioned among parties with an offline relationship or exhibiting certain security-based characteristics in order to protect the confidentiality, or indeed secret nature, of the transactions; but with additional public key distribution for some aspects of the supply chain to broaden and strengthen reliability of transaction credibility. The broader public participation could help ensure that there is an adequate number of distributed keys to validate transactions that don’t require the same level of confidentiality, while a parallel, smaller private ledger could be reserved for the most sensitive transactions.
To preserve DoD’s sensitivity to offshore data, it might be possible to distribute the blockchain network over domestic military bases with sufficient computing capacity to host the blockchain servers. That way there is a local copy of the ledger in case of network issues, and it is distributed in a way that there are no central points of attack.
This idea is not without its challenges. The use of blockchain for traditional industry logistics and accounting is still at the pilot stage. Its use demands significant technology expertise and server power and energy. Nor does this technology prevent human error, intentional corruption, or all security breaches.
All that said, other industries and countries are pioneering the use of blockchain to solve security, logistics management, and transactional cost challenges. The defense industry has begun to experiment with blockchain as a cybersecurity measure. It would be wise for the military to explore its uses elsewhere.
Elana Broitman is the director of New America NYC and a former Deputy Assistant Secretary of Defense in the Office of Manufacturing & Industrial Base Policy. She is on the advisory board of Notarytrade, a startup that offers blockchain-related services. Full bio
If interstate health plans become widespread, bare-bones plans with high out-of-pocket costs would proliferate
Interstate sales could make it harder for older and sicker adults to get adequate coverage at an affordable price
How would cross-state insurance work?
Under many Republican health reform proposals, insurance companies would be able to sell their policies across state lines. As long as a health plan complied with any one state’s regulations, that plan could then be sold nationwide—without necessarily complying with the regulations in every state.
What’s the backstory?
States have historically played a leading role in regulating health insurance. Prior to the 2010 enactment of the Affordable Care Act (ACA), state insurance regulations varied widely. States differed in the extent of medical underwriting they allowed, in their “guaranteed issue” requirements regarding people with preexisting conditions, and in permitting or preventing coverage denials for certain medical conditions. To sell policies in multiple states, insurers had to comply with each state’s insurance regulations.
The ACA created a more uniform system of rules for health insurers. The law provides a regulatory floor for health plans sold to individuals across all 50 states by requiring insurers to offer a plan to anyone who applies, prohibiting insurers from excluding coverage of preexisting health conditions, placing limits on what people can be charged based on their health, gender, or age, and requiring that every plan offer a set of “essential benefits,” such as preventive services and maternity care.
The ACA allows insurers to sell policies across state lines in states that have joined “health care choice compacts.”1 Six states—Georgia, Kentucky, Maine, Rhode Island, Washington, and Wyoming—have passed laws permitting such compacts. No states have joined them, and no insurers have expressed interest in selling plans in such an arrangement.2
How would cross-state insurance sales differ from current policy?
Republican reforms would eliminate most of the ACA’s national regulations, thereby making it easier for insurers to sell health insurance policies across state lines.
What are the basic arguments for and against cross-state insurance sales?
Conservatives believe allowing insurers to sell policies across state lines would inject competition into the individual market, which would lower costs for consumers.
Critics argue that if cross-state sales became widespread, the individual insurance market could become a race to the bottom. Insurance companies, they say, would relocate to states with the most insurer-friendly regulatory environments—in effect allowing national health care policy to be dictated by the most permissive states.
How would cross-state insurance sales affect costs and coverage for consumers?
If insurers sold plans across state lines, bare-bones catastrophic plans with low premiums and high out-of-pocket costs are likely to proliferate. These plans tend to appeal to younger, healthier adults who expect to use few health care services. This group may therefore see lower overall costs.
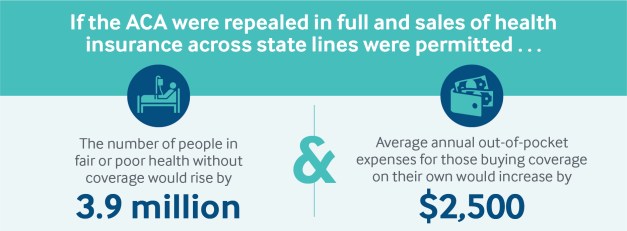
But as the young and healthy congregate in low-premium, high-deductible plans, insurers would become more reluctant to offer comprehensive policies. This would make it harder for older and sicker adults, who need more health care services, to obtain adequate coverage at an affordable price. With the remaining comprehensive plans attracting mostly sicker, costlier enrollees, premiums and out-of-pocket costs would increase sharply. RAND researchers estimate that average annual premiums overall could rise by as much as $2,500 a year if the ACA were repealed in full and cross-state sales were permitted.3
Cross-state sales of insurance are unlikely to otherwise produce any cost savings for consumers. Because out-of-state insurers have no current relationship or market share with in-state hospitals and physician practices, it would be difficult for these insurers to establish networks that can compete with established in-state carriers. This would make it hard for out-of-state insurers to negotiate sufficiently low payment rates to enable them to offer competitively priced plans. Out-of-state insurers would only be able to offer plans with higher premiums than their competitors, producing no net benefit to consumers.4
If the ACA were repealed, permitting insurers to sell policies across state lines would do little to offset the resulting coverage losses. According to RAND, in this scenario 17.5 million Americans would lose coverage, rather than 19.7 million under ACA repeal alone.5 And most of those gaining coverage through cross-state sales would be the young and healthy.
Nearly 3 decades ago, David Axelrod, MD, then commissioner of the New York State Department of Health (DOH), became concerned by the nearly 5-fold variation in cardiac surgery mortality rates across New York hospitals. Out of this concern, the DOH released the first public reports of surgical outcomes to the New York Times, labeling the performance of hospitals on cardiac surgical mortality rates across the state. After learning that individual surgeon mortality rates were also available, the Long Island–based Newsday sought release of the mortality rates of individual surgeons. The state demurred, arguing that data were less reliable at the surgeon level. Newsday quickly filed a Freedom of Information Act lawsuit to obtain the information and eventually prevailed in court, partly on the argument that patients generally choose surgeons, not hospitals.
This debate—whether it is best to report data on the hospital level only or whether to also report on individual surgeons—continues to this day. The evidence on whether the public or payers use these data to select high performers suggests that for the most part, they do not. But we do know that hospitals and physicians are paying attention. And there is widespread hope that with increasing consumerism in health care and with more patients paying out of pocket for their care, they will increasingly look for these kinds of reports.
That’s part of the reason public reporting is now so pervasive. While public reporting continues to become more common, how to report—whether to include only institutions or to also report on individual physicians—remains controversial. This debate was recently renewed when ProPublica, a highly regarded independent and nonprofit investigative journalist group, used national Medicare data to publish complication rates for hospitals and individual surgeons. It was their decision to name individual surgeons that was most controversial.
Criticism of Surgeon-Level Reporting
Critics of individual surgeon reporting have made a series of important arguments against the practice, each of which is worthy of consideration. And as more states and the federal government continue their efforts towards public reporting, these arguments against naming individual surgeons are gaining traction. But I believe that a careful examination of the literature indicates that moving away from surgeon-level reporting would be a critical mistake.
One common argument is that volumes of surgery for individual surgeons may be too low to be reliable. Small sample sizes can be a problem, but there are ways to address this issue. First, as New York State has done with cardiac surgery, one can aggregate performance across multiple years, thus substantially increasing sample size. Second, given that total volume of similar surgeries is also related to performance on a given surgery, (for example, a surgeon’s performance on esophagectomy improves with the number of other similar surgeries she performs) , one could use a surgeon’s performance across a range of procedures to increase sample size. Finally, publicly reported data could and should be presented with confidence intervals, to highlight the level of imprecision so that those reading the report are aware of the statistical limitations.
Critics of naming individual surgeons also argue that the practice would increase the likelihood that surgeons will avoid the hardest cases, thus reducing access to surgical care for the sickest patients. This is an important concern that has been voiced widely. However, the evidence on the extent to which this occurs is weak and anecdotal. Quite a few studies have tried to examine whether publicly reporting individual surgeon data leads to sicker patients not receiving care, and most have failed to find an effect. And to the extent that a few studies have found a reduction in access, these have been transient, with access returning to baseline within a couple of years of the reporting program.
Finally, and possibly most importantly, people who oppose reporting findings for individual surgeons have argued that much of medical care is now delivered in teams, and that each of the team members matters. They argue that naming an individual surgeon puts undue emphasis on that surgeon when the team’s performance is paramount. This argument is understandable; the importance of team work on surgical care is increasingly recognized. As the leader of the team, the surgeon plays a unique and outsized role, responsible for ensuring effective communication and well-delineated roles among team members, and for fostering a culture that supports team members speaking up when things have gone wrong. So when we publicly report a surgeon’s performance, we are essentially reporting on his or her surgical team’s performance.
Beyond Team Work
But even beyond team work, the empirical evidence of the importance of the individual surgeon’s role is overwhelming. Landmark studies have shown that within the same institution, there are large variations in outcomes across surgeons. Why might this be the case? It’s because outcomes of surgical care are influenced by a multitude of factors for which the judgment, skills, and capabilities of individual surgeons matter immensely.
Possibly the most consequential decision—whether to do the surgery at all—is undertaken primarily by the surgeon. Careful case selection—ensuring that the patient undergoing the procedure is likely to benefit—is critical to good surgical care, and reporting outcomes only at the institutional level would fail to capture the results of that judgment.
A second critical step in determining outcomes is the surgical technique itself. Recent studies have shown that there are large differences in basic surgical capabilities (from dissecting to cutting to suturing), and that highly skilled surgeons have dramatically better outcomes than less-skilled ones. The surgeon’s hands still matter. There are likely other factors that matter as well, but the empirical evidence is clear: picking the right surgeon is at least as important as picking the right hospital.
And that brings us to what is probably the most important reason to report data on individual surgeons: it’s information that patients want. When people seek advice on where to go for surgical care, they ask about the best surgeon for them. Telling the public that the surgeon doesn’t matter, that only the choice of hospital matters, is neither useful nor accurate. And it won’t work, because for patients, undergoing surgery creates deep anxiety, and trusting the judgment of an individual surgeon is paramount. Consumers would reject reports that only showcase institution-level data because they would find it less useful.
High Stakes
Publicly reporting on outcomes of individual surgeons is a high-stakes endeavor. We know from studies that some surgeons stopped practicing or moved away as a result of the New York State cardiac surgery reporting. There are still lingering fears that surgeons will turn away risky patients, although most surgeons have enough professionalism that they are unlikely to deny someone life-saving care just because it might hurt their rankings. But these fears mean we need to work harder at risk adjustment, and possibly create safe harbors for cases that are the highest risk.
But the surgeon remains critically important to surgery, and suggesting that what matters is the institution, not the individual, is both empirically inaccurate and unlikely to resonate with patients. We must address the challenges that come with individual surgeon-level reporting—not shy away from doing it. We must expand our efforts to report performance publicly, including for individual surgeons, not curtail them. Because if the goal is to improve surgical care, we must ensure that the person most influential in the process remains accountable for its outcome.
About the author: Ashish K. Jha, MD, MPH, is K. T. Li Professor of International Health and Health Policy at the Harvard T. H. Chan School of Public Health and a practicing internist at the Veterans Affairs Boston Healthcare System. He received his doctor of medicine from Harvard Medical School and was trained in internal medicine at the University of California, San Francisco. He received his master’s in public health from Harvard School of Public Health. Dr Jha’s major research interests lie in improving the quality and costs of health care. His work has focused on 4 primary areas—public reporting, pay for performance, health information technology, and leadership—and the roles they play in fixing the US health care system. (Image: Aubrey LaMedica/Harvard T.H. Chan School of Public Health)
About The JAMA Forum: JAMA has assembled a team of leading scholars, including health economists, health policy experts, and legal scholars, to provide expert commentary and insight into news that involves the intersection of health policy and politics, economics, and the law. Each JAMA Forum entry expresses the opinions of the author but does not necessarily reflect the views or opinions of JAMA, the editorial staff, or the American Medical Association. More information is available here and here.
 With the increasing
With the increasing 
 Jody Christ, in her home in Elysburg, Pa., says genetic testing saved her life, though experts warn such tests require caution.
Jody Christ, in her home in Elysburg, Pa., says genetic testing saved her life, though experts warn such tests require caution.