U.S. armed services are experimenting with ways to make faster — and smarter — decisions, and business should take note.

Article link: https://sloanreview.mit.edu/article/what-the-military-can-teach-organizations-about-agility
While the number of states contributing data was up from 18 to 49, challenges hindered CMS’ ability to effectively manage the program.
By Jessica Davis January 09, 2018 02:03 PM
 A lack of oversight of the national repository of Medicaid data caused an estimated $36.7 billion in payment errors in 2017, according to a new Government Accountability Office report. That’s up from an estimated $14.4 billion in improper payments in Fiscal Year 2013.
A lack of oversight of the national repository of Medicaid data caused an estimated $36.7 billion in payment errors in 2017, according to a new Government Accountability Office report. That’s up from an estimated $14.4 billion in improper payments in Fiscal Year 2013.
Transformed Medicaid Statistical Information System (T-MSIS) is CMS’ core effort to improve Medicaid data by increasing the scope of data and quality of state-reported data.
About 49 states began reporting that data to the national repository in November, up from just 18 states the year prior. The data help federal administrators to identify potential fraud and improve the efficiency of the program, but data aren’t sufficient enough for an effective oversight of the program.
[Also: Senators ask GAO for recommendations on unique patient identifiers]
“CMS has taken an important step toward developing a reliable national repository for Medicaid data,” the GAO report authors wrote. “However, data challenges have hindered states’ and CMS’s use of the T-MSIS data for oversight.”
For example, the reported data was incomplete for all of the selected six states reporting data in August 2017 as the states said that “certain unreported elements were contingent on federal or state actions and others weren’t applicable to the state’s Medicaid program.”
Further, states failed to mention in documentation whether those elements would be reported in the future, or when they would report complete data.
Six of eight selected states actually expressed concerns about how T-MSIS data could be compared across states. While all states reported interest in information sharing across states, CMS hasn’t compiled or shared information about states’ data limitation – an act that would help states improve accuracy when comparing data between states.
Although CMS has taken those first steps to using T-MSIS data, it doesn’t yet have a plan or even a timeframe to use this data for oversight.
“As a result, important CMS goals for T-MSIS, such as reducing states’ reporting burden and enhancing program integrity activities, are not being fully realized,” the report authors wrote.
GAO officials recommend CMS improve the completeness and comparability of T-MSIS data to accelerate the program, in addition to articulating a specific oversight plan.
The U.S. Department of Health and Human Services agreed with those recommendations and said it would continue to work on obtaining complete T-MSIS data from states. Further, the agency said it will take steps to address data sharing limitations within states, along with helping states collaborate.
“Strong Medicaid data can help the federal government and the states move toward better health outcomes and improve program integrity, performance, and financial management,” HHS officials told GAO, according to the report.
Twitter: @JessieFDavis
Email the writer: jessica.davis@himssmedia.com
 For any medical procedure, from a minor checkup to major surgery, there can be significant uncertainty about a key component: the price.
For any medical procedure, from a minor checkup to major surgery, there can be significant uncertainty about a key component: the price.
But what if there was greater transparency about the exact out-of-pocket price we would pay for a given procedure and how much that price varies across hospitals or providers? Would that change the providers we choose?
The answer is of interest to policymakers, whose goal is to encourage consumers to be more price-sensitive, saving money for themselves and reducing spending in the system overall.
“There’s a decades-long debate in healthcare about whether you can actually get people to shop on price,” says Elena Prager, an assistant professor of strategy at Kellogg. “We tend to view medical services as a different kind of product where price may not matter much.”
In a new study, Prager investigates whether consumers respond to simplified price information in choosing healthcare providers.
She finds that, indeed, price shopping in healthcare is possible—but it involves presenting consumers with price information in a much more simplified way than insurers typically do.
Do Healthcare Consumers Price Shop?
Think about your own healthcare bills for a moment. Do the words “simple” or “clear” immediately come to mind? Likely not.
“Even when people get an explanation of benefits from insurers, pricing can still be pretty opaque,” Prager says.
This is a problem because policymakers and insurers are trying to motivate consumers to understand the cost–benefit trade-offs of their healthcare decisions, as well as the value they are getting for the money spent—both out of their own pockets and from the balance sheets of insurers. But in most cases people lack the information to make informed decisions.
“On one hand, we’re asking for people to pay for more and more of their care” due to, for example, increasing deductibles and the rising cost of healthcare, Prager says. “But on the other, we’re not giving them the right tools to make good decisions about those large monetary amounts. So it’s important to understand whether it’s even possible to design effective healthcare price-information systems.”
Much of the earlier research on how to encourage price shopping in healthcare often focused on high-deductible health insurance plans.
“Even for care that serious, people are willing to trade off hospital prestige or distance to their house in order to save money.”
The logic was simple: if consumers have to cover a larger amount of their care—based on deductibles that could run well into the thousands of dollars before insurance coverage kicks in—they would be more price-sensitive when choosing services or providers.
But findings showed people had little sensitivity to price even when using these high-deductible plans.
“That’s because high-deductible insurance only solves one piece of the price-sensitivity problem by giving people more skin in the game,” Prager says. “These plans still don’t give enrollees sufficient price information. So people still have to figure out what the actual price they pay will be.”
That may mean finding and adding up prices from multiple medical areas and providers, even when considering only a single procedure. There may be different bills from the hospital and from the doctors working at the hospital, and from anesthesiology, surgery, the hospital pharmacy, and more. The information is often difficult to find, if not impossible.
The Simpler, the Better
Prager’s research used unusually transparent data from an insurance system in Massachusetts.
The study examined private health insurance claims from multiple insurers from 2009 to 2012. But importantly for the research, all these insurers gave consumers very clear information on cost.
Additionally, in many of the health plans, these insurers group hospitals into “tiers” based on price. A hospital’s tier determines consumers’ out-of-pocket payment for a given procedure at that hospital.
“For any procedure, such as a knee replacement,” Prager said, “people on these plans could look at insurer-provided documentation and on a single page see the price menu for all hospitals in the state, by tier—first, second, or third—and exactly what their out-of-pocket price will be. And it’s a set dollar amount, not 10 percent or 20 percent or the total cost. Just $300 or $700 or whatever, end of story.”
In some health plans, the difference in cost from one tier to another was substantial; for others, there was little to no price differential; and others simply had the same copay for all hospitals without using tiers. This allowed Prager to compare how consumers responded to the option to price shop in a very transparent system.
The data studied included the insurance plans of over 200,000 enrollees and dependents, the out-of-pocket prices they saw while making treatment decisions, and how much they and the insurers paid for procedures. The researchers focused on inpatient services—such as major surgery or delivering a baby.
The Power of Presentation
Prager found that people in the study did indeed opt for lower-priced medical services when presented with clear, simple price information.
For example, she modeled how the same patient would behave when enrolled in different types of plans—those with large cost differences between hospitals and those with none. She found that total spending per hospital stay fell by 1.3 percent when consumers were presented with cost differences.
Prager predicts that providers in the lowest-priced tier would gain about 53 percent in patient volume over three years due to price shopping.
“People weren’t sure price shopping in healthcare was even possible,” she says. “These findings show that it is.”
Indeed, people in the study were making price-based decisions about inpatient treatment, the type of higher-stakes interventions that required overnight stays.
“Even for care that serious,” Prager says, “people are willing to trade off hospital prestige or distance to their house in order to save money. So we might expect to see even greater price-shopping behavior for less serious care.”
Still, it takes an extremely simple approach to presenting price information to help people make healthcare decisions. “We haven’t been good at providing that in the US system,” Prager says.
Greater availability of simple healthcare price information would be good news for consumers and insurers alike. Patients save out-of-pocket costs by choosing lower-priced services, and insurers can save even more.
“Hospitals can differ by thousands of dollars for a given procedure,” Prager says, “and insurer savings can be many multiples of what consumers save when choosing a lower-priced option. Though not a guarantee, that might lower insurance premiums in the long run.”
What About Providers?
What are the implications of Prager’s findings for hospitals, physicians, and other providers?
“The level of enthusiasm providers have about these results will differ by where they are currently in the price distribution,” Prager says. She breaks down providers into three broad categories similar to the tiers insurers use.
Low-priced providers should be “thrilled” about price shopping, she suggests, because they can keep prices where they are and enjoy more volume because price-sensitive consumers will pick them when presented with clear price information.
Medium-priced providers are more likely to lose patient volume to lower-priced competitors because consumers will choose price over reputation or other factors such as proximity to home. “That will siphon off some volume from providers priced in the middle,” Prager says, “but they can try to negotiate lower rates with insurers in subsequent years to get into a lower tier.”
High-priced, highly desirable providers “won’t really care about price shopping,” Prager says, “because patients are willing to pay whatever it takes to get their care there.” She points to the Harvard-affiliated academic medical centers in the study as examples. These providers have such strong reputations that fewer consumers are willing to switch away from them, even if the price difference is stark. This means less savings for consumers and, especially, insurers.
The good news for patients and insurers is that the number of tiered insurance networks that have easier access to simple price information has grown in the last decade or so.
Over 10 percent of people enrolled in the Affordable Care Act exchange plans are in plans that are structured this way, Prager says, and a growing number of large employer-sponsored plans are, too. At the same time, many other insurers remain overly reliant on complex pricing tools, typically online, through which enrollees can search for providers and prices by procedure and zip code—but prices are still presented in a complicated way.
“Those complex tools are the darling of the industry,” Prager says, “but they don’t always work as well as hoped because they leave a lot of uncertainty about pricing. Instead, providing a simple menu of tiered-network options and prices has serious advantages that should be even more highlighted going forward.”
Article link: https://insight.kellogg.northwestern.edu/article/will-people-price-shop-for-healthcare
This chart collection takes a look at how spending on healthcare in the United States compares to other OECD countries that are similarly large and wealthy (based on GDP and GDP per capita). The analysis looks at 2015 health data from the OECD Health Statistics database. These charts are based on data from the OECD, allowing for international comparisons; however, some values from OECD are reported as provisional or estimated and may not exactly match U.S. data reported in the National Health Expenditure Accounts.
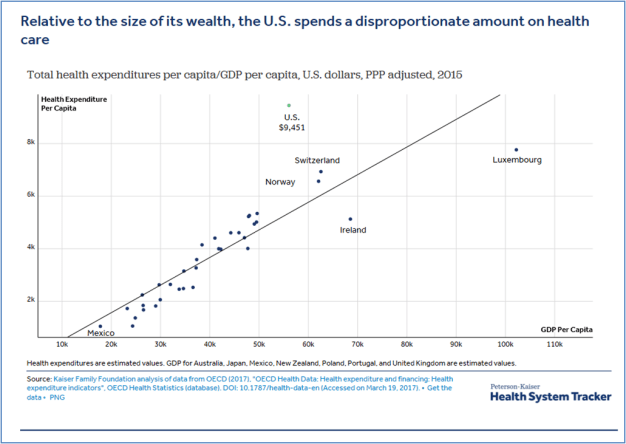
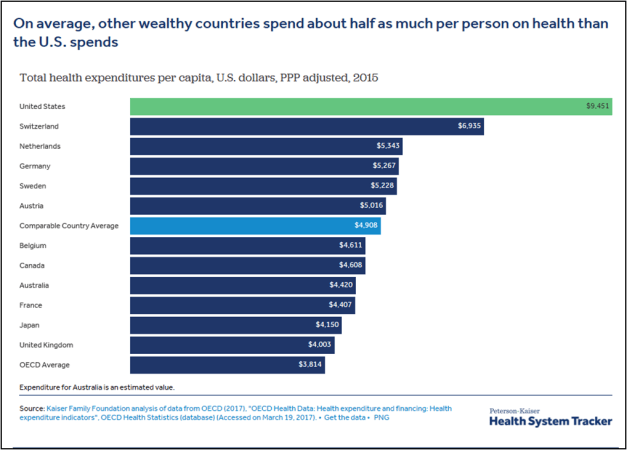
As would be expected, wealthy countries like the U.S., tend to spend more per person on health care and related expenses than lower income countries. However, even as a high income country, the U.S. spends more per person on health than comparable countries. Health spending per person in the U.S. was $9,451 in 2015 – 22% higher than Luxembourg, the next highest per capita spender.
Article link: https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries
The United States Health System Falls Short

Exhibit 1. Health Care Spending as a Percentage of GDP, 1980–2014
Source: OECD Health Data 2016. Data are for current spending only, and exclude spending on capital formation of health care providers.
The United States spends far more on health care than other high-income countries, with spending levels that rose continuously over the past three decades (Exhibit 1). Yet the U.S. population has poorer health than other countries. 1 Life expectancy, after improving for several decades, worsened in recent years for some populations, aggravated by the opioid crisis. 2 In addition, as the baby boom population ages, more people in the U.S.—and all over the world—are living with age-related disabilities and chronic disease, placing pressure on health care systems to respond.
Timely and accessible health care could mitigate many of these challenges, but the U.S. health care system falls short, failing to deliver indicated services reliably to all who could benefit. 3 In particular, poor access to primary care has contributed to inadequate prevention and management of chronic diseases, delayed diagnoses, incomplete adherence to treatments, wasteful overuse of drugs and technologies, and coordination and safety problems.
This report uses recent data to compare health care system performance in the U.S. with that of 10 other high-income countries and considers the different approaches to health care organization and delivery that can contribute to top performance. We based our analysis on 72 indicators that measure performance in five domains important to policymakers, providers, patients, and the public: Care Process, Access, Administrative Efficiency, Equity, and Health Care Outcomes.
Our data come from a variety of sources. One is comparative survey research. Since 1998, The Commonwealth Fund, in collaboration with international partners, has supported surveys of patients and primary care physicians in advanced countries, collecting information for a standardized set of metrics on health system performance. Other comparative data are drawn from the most recent reports of the Organization for Economic Cooperation and Development (OECD), the European Observatory on Health Systems and Policies, and the World Health Organization (WHO).
Article link: http://www.commonwealthfund.org/interactives/2017/july/mirror-mirror/
 A Hospital Charged $1,877 to Pierce a 5-Year-Old’s Ears. This Is Why Health Care Costs So Much.
A Hospital Charged $1,877 to Pierce a 5-Year-Old’s Ears. This Is Why Health Care Costs So Much.
An epidemic of unnecessary treatment is wasting billions of health care dollars a year. Patients and taxpayers are paying for it.

Article link: https://www.propublica.org/series/wasted-medicine
 Unused medical supplies sit in storage at a Partners for World Health facility in Portland, Maine. (Tristan Spinski, special to ProPublica)
Unused medical supplies sit in storage at a Partners for World Health facility in Portland, Maine. (Tristan Spinski, special to ProPublica)

This story was co-published with The Washington Post.
Squandered Health Care Dollars
In Maine, there’s a warehouse the size of a middle school gymnasium, stuffed with brand-new medical supplies and gently used medical equipment. Several pallets are piled with boxes of surgical sutures, still in their shrink wrap, each box worth hundreds of dollars. Tubs overflow with diabetes supplies and surgical instruments that may run hundreds of dollars apiece. There are bins of bandages and gauze and saline and ostomy bags and every other medical supply you can imagine. These materials, unexpired, could easily stock any hospital or clinic. But each item has actually been thrown away by a local medical facility.
The cost of health care has been rising for decades, and Americans are paying the price. In a recent Gallup poll, people cited the high cost of care as their No. 1 financial concern. It’s an enormous problem, and trying to solve it all at once brings on panic and paralysis. But after reporting for a year on the ways the medical industry blows through our money, I have one idea: Let’s end the egregious waste that’s draining our health care system.
The National Academy of Medicine has estimated the health care system wastes around $765 billion a year — about a quarter of what we spend. Eliminating all the waste could allow us to insure 150 million Americans, the Academy of Medicine said, and saving half of it could provide groceries for every household in the country for a year. Eliminating the waste would also stop our rising health care costs from eating up our wage increases. My premiums go up 9 percent next year. Same thing happened last year. Odds are your costs are rising, too.
It’s hard to downplay what I found when I began investigating the issue. Hospitals throw out so many valuable supplies that a cottage industry of charities has sprung up to collect this stuff and ship it to the developing world — otherwise, all those goods in that Maine warehouse would be headed for a landfill.
Nobody tracks how much hospitals waste rather than donate, and I couldn’t track down where each item came from. But experts told me when hospitals change vendors for a type of supply, they often toss the old stuff. Or, if they take over a clinic or facility, they get rid of the items that come with it, even if they are unused and unexpired.
The operating room is a major source of wasted spending. One hospital tracked the value of unused items that went to waste during neurosurgery procedures in a single year. The total: $2.9 million — for one type of surgery at just one hospital. In that case, the surgeons hadn’t updated their system of telling the staff which supplies to prep for each operation. They were opening many items they didn’t need, which then had to be thrown away even though they were unused. The hospital updated its approach to make sure they aren’t setting up for operations with excess supplies.
I learned that nursing homes throw away hundreds of millions of dollars’ worth of valuable medication every year. They typically dispense drugs a month at a time for patients and often have them discontinued if the patient dies or transfers. The excess drugs get trashed, incinerated or even flushed down the toilets, contaminating our water supply. The chief executive of a pharmacy that serves nursing homes in Florida told me that his company alone throws away about $2.5 million a year in valuable medication.
In Iowa, the state government funded a program to recover these castoff nursing home meds and donate them to needy patients, for free. This year, they’re on pace to recover and redistribute $6 million in medication. My story led policymakers in Florida and New Hampshire to introduce legislation to try to replicate the Iowa program.
Drugs are a huge source of waste, partly because drug expiration dates don’t mean what we think they mean. The Food and Drug Administration makes pharmaceutical companies show their medication is safe and effective until its expiration date. It doesn’t make them find out how long they actually last.
Studies show it’s common for a drug to be safe after its expiration date. The FDA runs a program that tests and then extends expiration dates on drugs in the federal government’s stockpiles. Those same drugs get thrown away in pharmacies when they “expire,” even though many of them are in short supply. How much of our money does it waste? One midsize hospital in Boston throws away about $200,000 worth of drugs a year that hit their expiration date. If that’s true for other hospitals, the total would be about $800 million a year for hospital pharmacies alone.
Meanwhile, drug companies are making eyedrops two or three times larger than what the eye can even contain. We are paying for the wasted medicine running down our cheeks. I spoke to the former head of research for Alcon Laboratories, a global leader in the eye care industry now owned by Novartis. He told me that in the early 1990s his team created a “microdrop” that eliminated the waste. The microdrops were effective and reduced the burning caused by larger drops. But Alcon’s leaders killed the project because they were worried it could reduce sales.
Vials of cancer drugs are also made too large, which one study said wastes about $1.8 billion a year in the valuable medication. Earlier this year, one drug company switched from a multiuse vial, which could be shared by patients, to a single-use vial that could not be shared, thereby increasing the amount of wasted cancer medication. The change would make the supply chain more reliable worldwide, the company said. But one cancer center calculated that the change would cost each patient an average of $1,000 in waste per infusion. Imagine: You’re fighting cancer and then get billed an extra thousand dollars for medication they toss in the trash. Two U.S. senators responded to my story by introducing legislation to solve the problem of oversized eyedrops and cancer drug vials.
These are not isolated examples or small sums being squandered. Let’s say my reporting identified about $10 billion in wasted spending. That’s a rough estimate because no one is actually tracking how much we’re wasting. What else could we be doing with that money? The Kaiser Family Foundation says it costs an average of $6,690 to pay one person’s insurance premium in 2017. At that rate, the $10 billion saved could insure about 1.5 million people for a year. Tell those people it isn’t important to reduce our wasted health care spending.
The Academy of Medicine did something smart when it reframed our health care overspending as waste. We may be a wasteful country, but we still teach our kids to eat everything on their plates. “Waste not, want not,” is baked into our cultural DNA. It’s a powerful concept because it’s a moral one. It’s wrong to squander the hard-earned dollars Americans are paying into the health care system and then demand they pay more.
We can’t be naive and think it will be easy to fix this problem. Our wasted spending represents revenue and profit for the medical industry. But our health care spending should not be an entitlement program for the medical industrial complex. I put together a prescription for reducing the wasted spending I identified. Our policymakers should stand up to the medical industry and stamp out the waste.
Article link: https://www.propublica.org/article/want-to-lower-health-care-costs-stop-wasting-our-money
Filed under: Health Care
Peter Kolchinsky, PhD
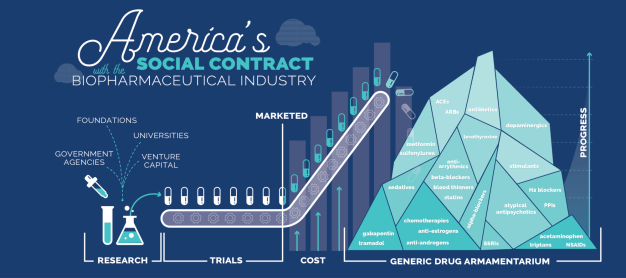
This is the first in a series of articles that aim to define the biopharmaceutical industry’s social contract with America, to examine practices that deviate from that contract, and to propose refinements to healthcare policy to ensure that our continued investment in scientific progress ultimately yields affordable, effective therapeutics for future generations.
Article 1: America’s Social Contract with the Biopharmaceutical Industry
Article 2: What happens when a drug won’t go generic?
Article 3: Protecting Off-Patent Sole-source Drugs from Price-Jacking
Please see Important Disclosures for Readers at the end.
The public has long voiced outrage at pharmaceutical companies over high drug prices. Many patients feel the real pain of rising healthcare costs and frequently call for price controls on prescription drugs. But price controls are not the solution. In fact, high prescription drug prices aren’t even the problem.
Miscast as a bloated expenditure, high prices on branded drugs incentivize and attract society’s talent and capital to the biopharmaceutical industry to fund and research new cures and treatments that will eventually become inexpensive generic drugs. These resulting generics are one of humanity’s most valuable and underappreciated resources.
High branded-drug prices are necessary to grow this mountain of inexpensive generic drugs. At the same time, we can’t allow anyone’s child or aging parents to be denied the medication they need on account of cost. The reason why new drugs seem unaffordable lies not with branded drug prices but with the intentionally poor design and distribution of healthcare insurance in our country. Branded drugs can be made more affordable — without imperiling biopharmaceutical innovation — by ensuring that insurance properly covers patients, sparing them the euphemism of cost sharing (e.g. co-pays and deductibles).
Besides shielding patients from drug costs and improving immediate health outcomes, this proposal will drive the scientific innovation needed to build a legacy of inexpensive treatments for future generations. Alongside other grand objectives like universal access to clean water and energy efficiency, building this mountain of useful generic drugs as rapidly as possible should be a national and global priority, one that America has led and should continue to lead. If we stall this engine of progress through price controls or other blunt measures meant to ease costs today, we condemn the future to be no better than the present. In turn, the biopharmaceutical industry should do its part to ensure all branded drugs are eventually and adequately genericized.
 While high-priced branded drugs make up only 11% of all prescriptions¹, they are the source of most pharmaceutical revenue ($237 billion in 2015²). Typically after 10–15 years, branded drugs lose their patent protection, unleashing low-cost generic versions³ (in 2015 the US spent a comparatively modest $88 billion on generics, though these drugs make up 89% of all prescriptions⁴). Unlike almost any other aspect of healthcare, drugs constantly go generic, which keeps total spending on retail drugs around a mere 12% of total healthcare costs, about the same as it was in 1972.⁵ And even though drug spending remains the same percent of overall healthcare spending, we now have far more and better treatments.⁶
While high-priced branded drugs make up only 11% of all prescriptions¹, they are the source of most pharmaceutical revenue ($237 billion in 2015²). Typically after 10–15 years, branded drugs lose their patent protection, unleashing low-cost generic versions³ (in 2015 the US spent a comparatively modest $88 billion on generics, though these drugs make up 89% of all prescriptions⁴). Unlike almost any other aspect of healthcare, drugs constantly go generic, which keeps total spending on retail drugs around a mere 12% of total healthcare costs, about the same as it was in 1972.⁵ And even though drug spending remains the same percent of overall healthcare spending, we now have far more and better treatments.⁶
Each year, the biopharmaceutical industry produces new drugs that raise our collective health, give hope to patients suffering from debilitating diseases, and further our understanding of human biology. Because the underlying biological processes inside our cells and bodies are essentially unchanging, the drugs we use today will work just as well in a hundred years, with few exceptions (e.g. antibiotics become obsolete and require replacement as bacteria evolve to become resistant). Many drugs may even work better with improved diagnostics, delivery technologies, and insight into how to best combine therapies. Therefore, much of the scientific progress we achieve in our lifetime will also accrue to the benefit of future generations.
Generics, which the FDA ensures work just as well and meet the same safety standards as original branded drugs, offer huge cost savings within months of coming to market and, with few exceptions, remain inexpensive for the rest of time.⁷
We need only look to the past to understand what progress can be made. Too often, we discount the ingenious tools for preventing, treating, and curing diseases that have made America and the whole world richer.⁸ Over the last hundred years, advancements in medicine, particularly perinatal care, vaccines, and antibiotics, as well as hygiene and nutrition contributed to the nearly 30 years added to the average American’s life expectancy.⁹ Over the same period, global life expectancy doubled.¹⁰ Quality of life also improved with groundbreaking treatments for heart disease, pain, diabetes, and many
 Cholesterol-lowering statins alone have contributed to the 50% decrease in death from both heart attacks and strokes throughout the developed world over the last few decades. When Pfizer’s patent on the best-selling statin Lipitor expired and generic versions entered the market, the price quickly dropped by 95% of the initial cost and has remained comparatively negligible ever since.¹² Gleevec, a highly successful drug that restores many years of life to patients suffering from chronic myelogenous leukemia (CML) and other cancers, has also recently gone generic, resulting in its price trending steadily downward. Today, our generic drug armamentarium includes treatments that manage blood pressure (ACEs, ARBs), cholesterol (statins, fenofibrate), diabetes (metformin, insulin), migraines (triptans, acetaminophen, NSAIDs), inflammation (steroids, methotrexate, 5-ASAs), chronic pain (gabapentin, tramadol), depression (SSRIs), schizophrenia (atypical antipsychotics), heartburn (H2 blockers, PPIs), hypothyroidism (levothyroxine), infections (antibiotics), enlarged prostate (alpha-blockers), insomnia (sedatives), ADHD (stimulants), Parkinson’s (dopaminergics), and cancers (anti-estrogens, anti-androgens, chemotherapies), as well as treatments that prevent heart attacks and strokes (blood thinners, anti-arrhythmics, beta-blockers). These represent just a glimpse of the medicines that biopharma can offer to humanity in this century if we continue to fuel and incentivize this industry.
Cholesterol-lowering statins alone have contributed to the 50% decrease in death from both heart attacks and strokes throughout the developed world over the last few decades. When Pfizer’s patent on the best-selling statin Lipitor expired and generic versions entered the market, the price quickly dropped by 95% of the initial cost and has remained comparatively negligible ever since.¹² Gleevec, a highly successful drug that restores many years of life to patients suffering from chronic myelogenous leukemia (CML) and other cancers, has also recently gone generic, resulting in its price trending steadily downward. Today, our generic drug armamentarium includes treatments that manage blood pressure (ACEs, ARBs), cholesterol (statins, fenofibrate), diabetes (metformin, insulin), migraines (triptans, acetaminophen, NSAIDs), inflammation (steroids, methotrexate, 5-ASAs), chronic pain (gabapentin, tramadol), depression (SSRIs), schizophrenia (atypical antipsychotics), heartburn (H2 blockers, PPIs), hypothyroidism (levothyroxine), infections (antibiotics), enlarged prostate (alpha-blockers), insomnia (sedatives), ADHD (stimulants), Parkinson’s (dopaminergics), and cancers (anti-estrogens, anti-androgens, chemotherapies), as well as treatments that prevent heart attacks and strokes (blood thinners, anti-arrhythmics, beta-blockers). These represent just a glimpse of the medicines that biopharma can offer to humanity in this century if we continue to fuel and incentivize this industry.
The collective armamentarium of branded drugs will mostly be generic within 10–15 years and will add to our high-value, low-cost arsenal. These include better treatments for many of the conditions mentioned above as well as breakthrough therapies or cures for cystic fibrosis, HIV, Hepatitis C, and many cancers. Yet so many problems remain to be solved. We must discover how to treat and cure diseases that run from uncomfortable to excruciating to devastating. Initially expensive, these drugs will soon enough go generic and join our growing mountain of cost-effective medications.¹³
Branded drug expenditures represent 1.8% of the US GDP.¹⁴ That’s a little more than a tenth of total healthcare spending and less than the 2.4% of GDP spent by the US government on roads, drinking water, and wastewater infrastructure, which few dispute as necessities worthy of investment.¹⁵ But because health insurance plans, including Medicare, engage in aggressive cost-sharing requiring co-payments as high as 20% of the price of a drug, vulnerable patients disproportionately carry the burden of building our common stockpile of generic treatments.¹⁶
Increased infrastructure investment stands as one of the last few areas of clear bipartisan agreement.¹⁷ We know that we need functional roads and water and sewage treatment facilities. We may even know that infrastructure spending will result in more jobs when Americans fix our roads and bridges.¹⁸ And yet, all this holds true for the drug industry: we all will eventually need what the millions of people employed directly or indirectly by the biopharmaceutical sector can create for us.
High-priced branded drugs power this entire biopharmaceutical ecosystem.¹⁹ Drug price controls would imperil it, signaling that some or even all the people involved should do something else for society, perhaps work in a different industry. Therefore, before we accidentally hobble or dismantle the biopharmaceutical industry in an effort to make today’s high-priced drugs cheaper as quickly as possible, we need ask whether branded drugs are “worth it” — essentially whether their price matches their value.
To understand a drug’s true value, consider each person that it will help as a branded drug in the present and as a generic in the future. Medicine has influenced every dimension of our lives, contributed to the advancement of art and technology that permeates our civilization by allowing innovators to live longer and healthier lives, and impacts our social fabric in immeasurable ways. Even a modest medical breakthrough that will someday go generic offers society high value for low cost.²⁰ We can collectively afford to make this investment.
This promise to create a mountain of low-cost therapies forms the core of the compact between drug developers and patients, which is to say all of us. Social contracts can be explicit, such as when Americans gave their representatives the power to govern them within the democratic precepts of the Constitution and the Declaration of Independence. In other instances, social contracts become implicit agreements between company and consumer. Google’s memorable motto “Don’t be evil” (now “Do the Right Thing”) became an implied promise to the user that “in exchange for using our services, we won’t do anything monstrous with the power you’ve given us.” Biotech operates on its own social contract with the American patient: “Yes, prices will be initially high on branded drugs. But after a patent expires, you enjoy the benefits of the cheap, effective generic versions for the rest of time.”
Others have proposed the notion of a social contract, notably with emphasis on keeping branded drug price increases in check while they are patent-protected.²¹ But as long as a drug ultimately will go generic, it’s not all that critical to the long-run price/value assessment whether it starts off at a lower price, climbs, and then goes generic, or if it starts off at a higher price, stays flat, and then goes generic.
Genericization without undue delays is the only critical feature of the contract. Consider the biopharmaceutical industry as putting novel branded drugs on a conveyer belt that over 10–15 years transports them to the top of the generic drug mountain– that final moment when the drug goes generic and falls off the conveyer onto the eternal generic mountain is the ultimate fulfillment of the industry’s end of the social contract.
There is more work to do in this regard. In the case of Gleevec, its price has been floating gently down after it went generic rather than fallen off a cliff, as Lipitor’s did. FDA approval of more generics would help speed the fall. In the case of biosimilars — which are as close as we can scientifically come to making a generic version of complex drugs such as antibodies and enzymes that are manufactured in biological systems — we are only just beginning to witness and assess the market dynamics around adoption and price erosion. But considering the cost of biologics production is in most cases roughly 5–15% of a biologic drug’s price, biosimilars may eventually be sold for at least a 70% discount. Companies will pursue every legal means at their disposal to prevent the uptake of biosimilars, as we have seen many innovators do to forestall generic entrants.²² The generics industry and the Federal Trade Commission estimate that America is losing out on almost $10 billion of savings each year due to such stall tactics, which is a problem and makes for many galling headlines, but it’s also less than 3% of total drug spend²³. Arguably the industry as a whole can afford to solve this public relations headache by swearing off excessive cleverness, and regulators should pursue avenues to accelerate genericization without impacting innovation, but regardless, those stall tactics fail in the long run and prices fall as competition sets in, as they have been steadily falling for Gleevec and its generics. For the few drugs where no true generic could ever exist — say, in the case of certain cell or gene therapies — new pricing mechanisms for the synthetic genericization of such drugs can and should be created, adapting pricing schemes already in place for pandemic vaccines and other biodefense products.
If we agree that the high prices of branded drugs legitimately drive investment towards society’s ownership of more and better generics, then we also need to condemn those who steal generics away from society. Making sure that drugs go generic and thereafter remain inexpensive is the long-term value side of the social contract. Therefore, when a company takes a formerly inexpensive generic and raises the price well above the cost of production without improving the drug, that company violates the contract. Several companies have recently exploited loopholes that regulators should seek to close quickly, for example by accelerating the approval of more generics to keep prices down and making sure that generic manufacturers can access samples of an original drug to help them demonstrate the equivalence of their generic product, both of which the FDA has vowed to do.²⁴
Imagine though, that all new drug development stopped, and all current branded drugs immediately went generic, for example through price controls or by invalidating their patents. Total drug spending would fall by approximately 70%, resulting in a one-time 9% reduction in healthcare spending, equating to about 1.5% of US GDP. Within a few years though, healthcare costs would revert to previous levels due to the rising costs of hospitals, surgeries, and other non-genericizable services.²⁵ Meanwhile, our mountain of generic drugs would cease growing — the conveyer belt will grind to a halt. Therefore, in exchange for a modest and temporary savings in our collective budget, we would destroy biopharma’s innovative core that, as of this moment, is advancing new treatments for migraines, bone fractures, cancer, diabetes, and countless other diseases that send patients, young and old, to hospitals each year. As overall costs continued to grow, the public would realize what Congress and insurance companies already know: the bulk of healthcare costs stem from hospitals and services, none of which will ever go generic.²⁶
Some argue that the biopharmaceutical social contract places responsibility on drug companies to make sure that patients have access to their drugs²⁷. This stance ignores the role of payers, private insurance companies as well as Medicare, in implementing high co-pays and other cost-sharing mechanisms to discourage patients from using medications that their physicians prescribe. The cost of most branded drugs could be cut in half and the majority of people in America still couldn’t afford to pay Medicare’s required 20% co-pay.
The tactics companies employ to try to make sure that patients can afford their share of the cost of a drug, such as co-pay assistance, are sometimes portrayed as bribes that companies pay patients to take their medications. Payers may worry that a pharmaceutical company has inappropriately marketed a drug, encouraging physicians to prescribe it to patients who don’t need it. When this happens, the government should prosecute and punish companies, but it’s inappropriate to cast suspicion on every doctor-patient interaction that results in a prescription for a high-priced drug and then, via cost-sharing, coerce patients into second-guessing their physicians. Many companies have programs to provide free drug to patients without insurance. And yet, many patients don’t realize that such programs exist, assume that they won’t be able to afford a drug, and don’t bother getting a prescription filled. Physicians are often too busy to explain the details of co-pay assistance to each patient. These barriers to access create their intended result: fewer patients fill prescriptions that their physicians write.
We have also entrusted our government and insurance companies to distribute the costs of healthcare across our population and across time so that people unfortunate enough to be sick don’t suddenly find themselves choosing between the branded drugs they need and their mortgage payments. Insurance practices in America conform to laws passed by our elected representatives. So if the politicians we elect to Congress allow insurance companies to turn away people based on pre-existing conditions or to charge high co-pays, then we have harmed ourselves.
A common complaint is that healthcare is more expensive in the US than anywhere else in the world but that our outcomes lag far behind.²⁸ This has little if anything to do with pharmaceuticals. On the contrary, the US enjoys faster approvals of innovative drugs, giving many US patients access to important medicines, such as cures for hepatitis C, years before they are used widely in Europe.²⁹ At the same time, the US makes the most use of generic drugs — more than any major healthcare market. While 89% of prescriptions filled in the US are for generics, throughout Europe generic utilization remains far lower, from Switzerland (17%) to France (30%) to Spain (47%) to Germany (80%).³⁰ Therefore, although Europeans pay less than Americans for branded drugs initially, they pay branded prices for longer because they don’t switch to generics as quickly as possible. As much as it is popular to cite how much more the US pays for a new drug, there are also many examples of older drugs for which Europe pays more. While the US has already cured many patients suffering from hepatitis C, for example, Europeans are spending more money on older, less effective treatments.³¹ Despite having the most advanced technologies, the US system, through cost-sharing, non-comprehensive insurance, and bureaucracy, makes healthcare unaffordable and practically inaccessible for some, which then weighs on healthcare outcomes for these individuals and also shows up in national statistics.³²
Copays and deductibles imposed upon patients force many to stop taking their medications as prescribed, leading to worse outcomes and higher long-term costs. Even small co-pays and fees — as low as $1 to $5 — reduce drug adherence and cause patients to avoid necessary care.³³ Approximately 50% of patients fail to adhere to their prescriptions due in part to high co-pays, while high deductibles push patients to cut out valuable preventative services. Greater cost-sharing is also associated with increased emergency room visits.³⁴ Low-income patients are often the most vulnerable. Indeed, the very term “cost-sharing” disguises what could be more aptly described as an institutionalized failure to insure.
If we truly hope to expand access and unburden patients of the financial hardship of getting sick, then rather than blaming the innovators for the prices of their newest drugs, let’s upgrade our insurance system to one that actually provides proper insurance to everyone. Spending should be spread more evenly instead of hitting patients with toxic cost-sharing when they are sick and most vulnerable. Cost-sharing just adds insult to injury. Imagine if, after being mugged, the victim had to make a co-pay to have the police show up.
Cutting out-of-pocket costs would lead to improved adherence, better health outcomes, and lower long-term healthcare spending, provided that physicians do not encourage patients to over-utilize an “all you can eat” healthcare system. While this is an important caveat, it does not justify cost-sharing, which shifts the responsibility of setting an appropriate level of care from knowledgeable physicians to distressed patients. Co-pays and deductibles are intended to make sure that individuals have some “skin in the game” and think twice before seeking unnecessary treatments. However, few patients can tell the difference between a necessary and unnecessary treatment when the person prescribing the treatment is a doctor.
If a doctor prescribes an expensive branded drug despite the availability of generics or less expensive but similar therapies, it makes sense to nudge patients towards switching. The problem is when payers try to discourage patients from taking uniquely beneficial drugs for which there are no substitutes. Behavioral economists conceded long ago that humans do not always behave rationally, often undervaluing their future selves. When insurers place significant cost burdens on a patient, they nudge individuals to indiscriminately reduce their use of both low-value and high-value treatments and services, often with costlier downstream consequences.
Specific private and government insurance practices were designed with high co-pays, maybe thoughtlessly or maybe heartlessly, to make patients believe that drugs are unaffordable. Yet, the 1.8% of GDP that America spends on branded drugs does not have to feel unaffordable to any of the people who need these medications, just as our nation’s road and drinking water infrastructures are considered a basic resource available to all.
Insurance companies should address overutilization of services and unnecessary prescriptions by confirming that physicians adhere to standard of care guidelines, not by underinsuring patients so they are financially discouraged from following their doctors’ advice. And insurers should align physician incentives with the quality of care rather than the quantity of care. Fortunately, there are many ongoing experiments being run by hospitals, physician networks, and insurers to figure out how to do just this.³⁵
Insurance only serves its function if everyone, especially healthy people, pays what they can. Just as taxes grow in proportion to income, insurance companies should ensure that an individual pays their highest rates during their highest income years, which also happens to be when they are younger and most likely to be healthy. It makes little sense to increase costs on people when they are older, have less income, and yet are most likely to need healthcare. The young, healthy, working-age population might not like paying more, but they will eventually find themselves in need of the medicines whose development they helped fund while they were younger. Until insurance functions properly, patients driven to desperation by cost-sharing will understandably find government-imposed drug-price controls appealing, regardless of the consequences to the biopharmaceutical ecosystem.
There has always been difficulty establishing a drug’s cost-effectiveness, a quantification of whether it is “worth it”. One can make the case that a patient with elevated cholesterol who skips treatment to save money will only end up costing himself, his family, and society more if he later suffers a heart attack, and that, therefore, the patient and society should rationally want the patient to get preventative treatment. However, the cold hard math of dollars spent and saved does not always support this conclusion because it depends on the cost of the treatment and the value one places on life. An oft-cited macabre bit of trivia is that smokers save taxpayers’ money on Medicare and Social Security by dying more quickly and earlier than non-smokers. If it were all about money, we should be encouraging smokers to keep lighting up. But we are using a calculus that heavily weighs well-being, which basically means that the benefits of healthcare are unquantifiable, at least in America. As a society, we have not come to terms with how to put a price on life (one could argue that the EPA sets the value of a statistical life at $10M in 2016, FDA just under at $9.5M, and the Department of Agriculture at $8.9M³⁶) and seem to believe that paying whatever it takes to treat or prevent pain, disability, and death is always the “right” choice, or at least the American choice. Anyone who puts money over life is considered heartless.
Yet we know that our inability to say “no” to effective medications on the basis of cost makes us vulnerable to price gouging, and we know that drug companies know this, calling into question whether drug companies are charging a “fair” price, even as we struggle to define what fair is. Some would argue that fair means pegging prices to the cost of drug development, calling for every company to disclose what it cost them to develop each drug. Others suggest it’s only fair to charge for a drug if it works, although in practice we often do not know if a drug is working for a specific patient.
Neither of these suggestions would be impossible to implement in some form and, through transparency, might even help make drug development more efficient. The drug industry’s profit margins are roughly 20%, which some say are too high. But we know that there isn’t room to reduce branded drug prices by half, for example, at least not without cutting salaries and laying off people. There are no doubt inefficiencies in every company, but which specific expenses are unnecessary is debatable. Profit margins appear modest for an industry accused of being a price gouging monopoly.
There is a good chance that, after every R&D expense has been audited by Congress and when companies are only allowed to charge for drugs that work, the industry will be found to be justified in charging a collective 1.8% of US GDP for branded prescription drugs. Where would the public outrage then turn? Maybe it will finally turn where it needs to focus, on the lack of universal insurance in America and the heartless practice of imposing cost-sharing on the sick and vulnerable. Inadequate insurance coverage and high co-pays are at the root of why patients go without. Insurance companies and government policies are standing in the way of patients accessing medications that could help them.
There would be less outrage if patients could count on their insurance plans to pay in full for whatever drug their physicians prescribed. Controlling the prices of the more expensive branded drugs is counter-productive and, in the long run, irrelevant, as long as those drugs will go generic.
The central element of the biopharmaceutical social contract, as we see it, has little to do with what price is fair for a branded drug. That’s an unwinnable debate and a search for unquantifiable value. Instead ask whether or not a drug will eventually go generic, offering society reassurance that there is an end in sight to the high cost of any new drug. Basically, whatever the branded price, that high cost is finite, whereas the value society will enjoy is infinite. Some might think that hepatitis C drugs approved since 2015 were indisputably overpriced, yet when the first hepatitis C drugs came to market, the public outcry over their high cost for a short course of treatment was hardly universal. Many articles pointed to how much more cost-effective these curative drugs were compared to previous HCV therapies or HIV medications that cost less but must be taken chronically. And the more productive the biopharmaceutical industry has become, the more likely it is that multiple competitors come to market with comparable drugs within a few years of one another, spurring some price competition even before generics set in, as has happened with treatments for hepatitis C, diabetes, and cholesterol management. It’s increasingly rare for any drug company to enjoy a monopoly for very long.
Indisputable price-gouging, like price-jacking an old generic drug, does happen, but on a comparatively small scale. These practices can and should be eliminated (the FDA has already taken steps to do so by approving generics more quickly). There may even be a role for price controls by having the government contract with manufacturers of old single-source generics (i.e. those supplied by just one company, usually because the residual demand for these older drugs is too small to sustain multiple competitors), ensuring a continuous supply at a modest profit margin.
Populist demands to cut drug prices may tempt some, but the innovative edge of the pharmaceutical industry is powered by the willingness of the US market to reward groundbreaking research. Even European pharmaceutical companies would likely not bother investing in the development of many kinds of new drugs if they couldn’t count on selling them in the US. Hitting the biopharma industry with price controls in reaction to understandable but misdirected outrage would only rob ourselves and our children of the compounded growth of our giant mountain of generic drugs. If we conflate investing in new drugs that we will someday “pay off” with simply spending money on expensive healthcare services (which never go generic), then we may make the wrong budget cuts and thereby only worsen our long-term costs and outcomes.
Consider a home mortgage. A borrower spends 15–30 years paying off a mortgage, typically while younger and employed. Those mortgage payments can be substantial, but once the house is paid off, it is lived in rent free and then passed down to children and grandchildren. By comparison to drugs, doctors, surgeries, and treatments such as dialysis are pure rent and will remain expensive forever — we can only hope to prevent the need for these expensive services with inexpensive drugs.³⁷ A heart bypass and a cardiac surgeon may never go generic, but cholesterol lowering statins, which prevent hospital admissions and even surgeries, will be cheap indefinitely.
When President Kennedy proposed that Americans send a man to the moon, he asked the country to boldly commit to a goal that would require substantial funding, partnerships between government and corporations, and immense intellectual capital. He explained that “in a very real sense, it will not be one man going to the moon — if we make this judgment affirmatively, it will be an entire nation. For all of us must work to put him there.”³⁸ Individual scientists and research teams will be the ones to discover the next generation of cures and treatments, but their successes will be the product of a collective societal effort. Just as the Apollo Program produced breakthroughs in engineering, computing, and our understanding of spaceflight, let us recognize that the high cost of today’s new drugs fuels and inspires the continued discovery of tomorrow’s medical advances, providing high-value, affordable generics that will benefit us all for the rest of time.
Acknowledgements: I’m grateful to Aaron Hiltner and Chris Morrison for their invaluable and substantive thought-partnership and drafting/editing and to everyone who engaged with me in the constructive debates that led up to this article.
Article link: https://medium.com/the-biotech-social-contract/kolchinsky-tbsc-1-dafc2fe803e5
¹ http://www.gphaonline.org/media/generic-drug-savings-2016/index.html.
² https://www.cdc.gov/nchs/data/hus/hus16.pdf#094; http://www.gphaonline.org/media/generic-drug-savings-2016/index.html.
³ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4899342/.
⁴ http://www.gphaonline.org/media/generic-drug-savings-2016/index.html.
⁵ https://data.oecd.org/healthres/pharmaceutical-spending.htm; https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/highlights.pdf.
⁶ http://content.healthaffairs.org/content/23/1/10/F1.expansion.html; https://www.cdc.gov/nchs/data/hus/hus16.pdf.
⁷ http://www.nejm.org/doi/full/10.1056/NEJMp1704907?af=R&rss=currentIssue#t=article.
⁸ https://data.oecd.org/healthstat/potential-years-of-life-lost.htm;
https://data.oecd.org/healthstat/life-expectancy-at-birth.htm#indicator-chart.
⁹ http://u.demog.berkeley.edu/~andrew/1918/figure2.html; http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/atlas.html; http://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2626194; https://ourworldindata.org/life-expectancy/.
¹⁰ http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/atlas.html; https://ourworldindata.org/life-expectancy/.
¹¹ http://u.demog.berkeley.edu/~andrew/1918/figure2.html; http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/atlas.html; http://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2626194; https://ourworldindata.org/life-expectancy/
¹² https://hbr.org/2014/11/the-real-cost-of-high-priced-drugs
¹³ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4899342/
¹⁴ The most recent figures come from 2015. In 2015, the U.S. spent $325B on retail drugs and an estimated $128B on non-retail drugs, for a total of $453B. For retail drugs, branded drugs made up 73% of all spending. If we apply the same estimate to non-retail drugs, we see that the U.S. spent $331B on branded drugs. The U.S. GDP was $18.0366T in 2015, leading to a calculation of 1.8%. https://www.cdc.gov/nchs/data/hus/hus16.pdf#094; https://aspe.hhs.gov/system/files/pdf/187586/Drugspending.pdf; http://www.gphaonline.org/media/generic-drug-savings-2016/index.html.
¹⁵ From the above footnote we see that the U.S. spent $331B on branded drugs. The U.S. spent $3.2056T on healthcare. $331B/$3.2056T = 10.3%. See https://www.cdc.gov/nchs/data/hus/hus16.pdf#094. For GDP spent on roads, drinking water, and wastewater infrastructure see https://www.cbo.gov/publication/52463.
¹⁷ http://i2.cdn.turner.com/cnn/2017/images/03/08/rel4d.-.budget.pdf.
¹⁹ http://www.gphaonline.org/media/generic-drug-savings-2016/index.html.
²⁰ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4899342/.
²¹ https://www.allergan.com/news/ceo-blog/september-2016/our-social-contract-with-patients.
²² https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4899342/
²³ http://www.gphaonline.org/media/cms/REMS_Studyfinal_July2014.pdf; https://www.ftc.gov/sites/default/files/documents/reports/pay-delay-how-drug-company-pay-offs-cost-consumers-billions-federal-trade-commission-staff-study/100112payfordelayrpt.pdf
²⁵ https://data.oecd.org/healthres/health-spending.htm; https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/Proj2015.pdf.
²⁸ http://www.nejm.org/doi/full/10.1056/NEJMp1708704
²⁹ http://www.who.int/intellectualproperty/events/en/R&Dpaper2.pdf; http://eprints.lse.ac.uk/71641/7/Wouters_Comparing%20generic%20drug%20markets_2017_author%20LSERO.pdf
³⁰ http://www.gphaonline.org/media/generic-drug-savings-2016/index.html; http://eprints.lse.ac.uk/71641/7/Wouters_Comparing%20generic%20drug%20markets_2017_author%20LSERO.pdf
³² http://www.commonwealthfund.org/publications/in-the-literature/2016/nov/2016-international-health-policy-survey-of-adults; http://www.nejm.org/doi/full/10.1056/NEJMp1708704
³⁴ https://jamanetwork.com/journals/jama/fullarticle/1108322
³⁵ http://catalyst.nejm.org/simple-case-health-insurance-complexity/ ; http://www.choosingwisely.org/
³⁶ https://www.bloomberg.com/graphics/2017-value-of-life/
³⁷ http://www.nbcnews.com/health/health-care/surgery-prices-surge-innovation-consolidation-under-obamacare-n191901 ; https://hbr.org/2014/11/the-real-cost-of-high-priced-drugs
³⁸ https://www.nasa.gov/vision/space/features/jfk_speech_text.html
Peter Kolchinsky is a founder, Portfolio Manager, and Managing Director at RA Capital Management. Peter is active in both public and private investments in companies developing drugs, medical devices, diagnostics, and research tools, and serves as a Board Member for various public and privately held companies, including Dicerna Pharmaceuticals, Inc. and Wave Life Sciences Ltd. Peter also leads the firm’s outreach and publishing efforts, which aim to make a positive social impact and spark collaboration among healthcare stakeholders, including patients, physicians, researchers, policy makers, and industry. He authored “The Entrepreneur’s Guide to a Biotech Startup” and served on the Board of Global Science and Technology for the National Academy of Sciences. Peter holds a BS from Cornell University and a PhD in Virology from Harvard University.
The opinions in this article are my own, subject to change, and may not reflect the opinions of RA Capital Management or anyone with whom I am affiliated. With regard to data and anything presented as fact, I’ve made an effort to be accurate and cite sources I believe to be accurate, but it’s possible I’ve erred or that my sources were inaccurate, in which case hopefully not in ways that materially impact the overall argument. If you think you’ve spotted an error, please contact me to help me improve my reasoning. While you probably already know this, regulations I’m beholden to as an investor nonetheless require me to remind you that nothing may turn out the way I want things to or predict that they might in this article, whether with a company, the healthcare system, or the economy in general. This article may reference specific companies to provide real-world examples of otherwise generalizable abstract concepts; nothing in this article is intended to be taken as investment advice in any company or in my firm. To help you judge my conflicts of interest, let me draw your attention to the possibility that I or my firm may have invested, may be invested, or someday may invest in the securities of companies mentioned in these articles. If I or my firm have a relationship or investment position in any company mentioned in an article, that would be specifically disclosed in the text of the article at the time of publication and will be accurate as of the time of initial publication but may change thereafter.
On the last week of April earlier this year, a small committee of doctors met quietly in a midsized ballroom at the Renaissance Hotel in Chicago. There was an anesthesiologist, an ophthalmologist, a radiologist, and so on—thirty-one in all, each representing their own medical specialty society, each a heavy hitter in his or her own field.
The meeting was convened, as always, by the American Medical Association. Since 1992, the AMA has summoned this same committee three times a year. It’s called the Specialty Society Relative Value Scale Update Committee (or RUC, pronounced “ruck”), and it’s probably one of the most powerful committees in America that you’ve never heard of.
The purpose of each of these triannual RUC meetings is always the same: it’s the committee members’ job to decide what Medicare should pay them and their colleagues for the medical procedures they perform. How much should radiologists get for administering an MRI? How much should cardiologists be paid for inserting a heart stent?
While these doctors always discuss the “value” of each procedure in terms of the amount of time, work, and overhead required of them to perform it, the implication of that “value” is not lost on anyone in the room: they are, essentially, haggling over what their own salaries should be. “No one ever says the word ‘price,’ ” a doctor on the committee told me after the April meeting. “But yeah, everyone knows we’re talking about money.”
That doctor spoke to me on condition of anonymity in part because all the committee members, as well as more than a hundred or so of their advisers and consultants, are required before each meeting to sign what was described to me as a “draconian” nondisclosure agreement. They are not allowed to talk about the specifics of what is discussed, and they are not allowed to remove any of the literature handed out behind those double doors. Neither the minutes nor the surveys they use to arrive at their decisions are ever published, and the meetings, which last about five days each time, are always closed to both the public and the press. After that meeting in April, there was not so much as a single headline, not in any major newspaper, not even on the wonkiest of the TV shows, announcing that it had taken place at all.
In a free market society, there’s a name for this kind of thing—for when a roomful of professionals from the same trade meet behind closed doors to agree on how much their services should be worth. It’s called price-fixing. And in any other industry, it’s illegal—grounds for a federal investigation into antitrust abuse, at the least.
But this, dear readers, is not any other industry. This is the health care industry, and here, this kind of “price-fixing” is not only perfectly legal, it’s sanctioned by the U.S. government. At the end of each of these meetings, RUC members vote anonymously on a list of “recommended values,” which are then sent to the Centers for Medicare and Medicaid Services (CMS), the federal agency that runs those programs. For the last twenty-two years, the CMS has accepted about 90 percent of the RUC’s recommended values—essentially transferring the committee’s decisions directly into law.
The RUC, in other words, enjoys basically de facto control over how roughly $85 billion in U.S. taxpayer money is divvied up every year. And that’s just the start of it. Because of the way the system is set up, the values the RUC comes up with wind up shaping the very structure of the U.S. health care sector, creating the perverse financial incentives that dictate how our doctors behave, and affecting the annual expenditure of nearly one-fifth of our GDP.
It’s fairly common knowledge at this point that Congress does not allow Medicare to negotiate with pharmaceutical companies over the amount the government pays for their drugs. Each drug company simply sets a price for its own product, and Medicare either takes it or doesn’t. While that arrangement undoubtedly drives up Medicare spending—and health care spending more generally—it at least allows for some competition among the drug companies that manufacture similar products. But when it comes to paying doctors for the services and procedures they perform, the system is even more backward. In this case, Medicare actually asks the suppliers—the doctors themselves—to get together first, compare notes, and then report back on how much each of them ought to get paid.
Medicare is not legally required to accept the RUC’s recommended values for doctors’ services and procedures, but the truth is, it doesn’t have much of a choice. There is no other advisory body currently capable of recommending alternative prices, and Congress has never given the CMS the resources necessary to do the job itself.
The consequences of this set-up are pretty staggering. Allowing a small group of doctors to determine the fees that they and their colleagues will be paid not only drives up the cost of Medicare over time, it also drives up the cost of health care in this country writ large. That’s because private insurance companies also use Medicare’s fee schedule as a baseline for negotiating prices with hospitals and other providers. So if the RUC inflates the base price Medicare pays for a specific procedure, that inflationary effect ripples up through the health care industry as a whole.
Another, even more powerful consequence of this system is that while the prices Medicare and private insurers pay for certain procedures have increased—sometimes rapidly—the prices paid for other services have declined or stagnated. That’s largely because of basic flaws in the way the system is set up. For one, the RUC spends the vast majority of its time reviewing specialty procedures, which change more quickly as technology advances, rather than so-called “cognitive” services, like office visits, that primary care doctors and other generalists rely on for the bulk of their income. The result is that there are “a hundred ways to bill for removing varicose veins, and only one way to bill for an intermediate office visit,” one former RUC member told me. For another, the RUC is dominated by specialists, who have a direct interest in setting the reimbursement rates for specialty procedures much higher than for general services.
Those two factors go a long way toward explaining why we’ve seen an explosion of billing for certain types of lucrative procedures. After all, the incentives are perfectly aligned: ordering that extra test means more money for a doctor’s practice or hospital, more money for the labs, and often more money for the device makers and drug companies, too. (Oh, and, by the way, the device makers and drug companies are, not incidentally, major funders of the medical specialty societies whose members vote on the RUC.)
These manipulated prices are also a major reason why specialists are in oversupply in many parts of the country, while a worsening shortage of primary care providers threatens the whole health care delivery system. It’s precisely because the RUC has overvalued certain procedures and undervalued others that radiologists now make twice what primary care docs do in a year—that’s an average of $1.5 million more in a lifetime. While that little fact doesn’t explain everything (doctors choose their fields for a multiplicity of reasons), future income is, presumably, not entirely unimportant to a young MD.
And we’re not just talking about medical students here. Having the wrong kinds of doctors in the wrong places, with the wrong financial incentives, is one of the major reasons why Americans pay so much more for health care than do citizens in other advanced nations, and yet we live no longer.
Over the past few years, a few well-placed health care figures from both parties have spoken out—at least once they’ve left office—about how crazy this system is. “The RUC is really just a giant cabal run by the AMA,” Thomas Scully, former head of the CMS under George W. Bush, told me. “A private trade association should not have that sort of control over the biggest spending account in the government. It’s an outrageous travesty of democracy.” Bruce Vladeck, former head of the CMS under Bill Clinton, agrees, calling the RUC “a significant part of the problem.”
There have also been scathing reports issued by the Government Accountability Office, and by MedPAC, the agency that advises Congress on Medicare-related issues, as well as some hard-hitting investigative reporting by the Wall Street Journal and the Center for Public Integrity. In 2011, a bipartisan panel participated in a Senate roundtable, during which three former heads of the CMS took turns lamenting the RUC.
Yet, for the most part, the RUC continues to operate exactly as it always has—behind the scenes, without anyone, including actual doctors laboring in the clinics and hospitals across the country, even really knowing about it. (This spring, Scully told me that he went to lunch with a very high-ranking official at the CMS who had no idea how the RUC actually worked.)
The Affordable Care Act, for its part, includes a few lines that could potentially, if incrementally, limit the RUC’s power. But in general, it doesn’t much change the way the reimbursement system works. Taking on the RUC would have “started a nuclear war with the AMA,” as Scully put it, and alienated other key political allies that the administration needed to pass the law to begin with. Fixing the RUC, however, is essential to fixing health care in this country.
“Follow the money,” said Gail Wilensky, who headed the CMS under George H. W. Bush and has been critical of the RUC. “Change the way physicians are paid, and you change the system.”
The RUC, like that third margarita, seemed like a good idea at the time. When liberals were trying to pass Medicare in 1965, the staunchest opponent they faced was the AMA, which was dead set against the program on the grounds that “socialized medicine” would upend physicians’ livelihoods.
In order to get the bill passed, liberals made many big concessions to organized medicine. One was keeping the “fee-for-service” payment system, which we still have today, in which doctors bill Medicare (and private insurance companies and uninsured patients) according to every single service or procedure they perform. Another was that Medicare promised to pay physicians the “usual, customary and reasonable” rate for each of those services. One of the problems that quickly arose was that there was no benchmark for what was “usual” or “reasonable,” no nationally accepted standard for “customary” for the price of each individual service or procedure. Prices, unsurprisingly, began to skyrocket.
Someone who worked with the Bush administration in the 1980s told me a story about an ophthalmologist in Texas, known as the legendary “Cataract King.” Despite the fact that a cataract surgery had gotten much easier to perform—it took two to three hours when it was first invented, but by the ’80s clocked in at about a half an hour—he continued to charge the “customary” rate: up to $6,000 a pop. By the mid-’80s, Medicare was spending about 4 percent of its budget on cataract surgeries alone. Meanwhile, an hour-long visit with a patient resulting in a complex diagnosis fetched about forty bucks.
By 1985, doctors’ rates were, to say the least, wildly distorted and Medicare spending was outstripping the growth of both the economy and federal tax receipts year after year. Panicked, Congress amended the law in 1986 to require doctors to charge Medicare according to “historical” rates, but it was too little too late. “Historical” rates were already crushingly high, and Medicare was on the verge of collapse.
And that’s when Harvard economist William Hsiao entered the scene. In 1988, he and his team unveiled what they hoped would be a rational process for setting physicians’ reimbursement rates. The result came to be known as the resource-based relative value scale (RBRVS). By interviewing hundreds of doctors from dozens of specialties, they painstakingly compared thousands of medical procedures—everything from removing a polyp to a lung transplant—and assigned each a relative value unit (RVU) according to three main factors: one, the amount of work it takes for a doctor to perform a given procedure; two, a doctor’s practice costs; and three, malpractice liability. Every year, Congress then sets a multiplier, converting that RVU into dollars.
At the end of 1989, as part of the Omnibus Budget Reconciliation Act, Congress formally adopted Hsiao’s system, requiring that Medicare use the RBRVS in determining the prices it paid physicians. It went into effect in 1992.
The plan went downhill almost immediately. In order for the system to work in practice, new services and procedures had to be added and old ones updated every year. Certain procedures, like in the cataract surgery example, that were initially very difficult and time-consuming to perform had become steadily more routine and quicker to do, while other procedures had gotten more complex and required more skill to perform. Those RVUs needed to be adjusted accordingly. The question soon became: Who should be responsible for updating the RVUs for all those thousands and thousands of procedures?
The Bush administration, skittish of anything resembling government price setting, rejected the idea of establishing an independent council of advisers within the government. Instead, in 1991, they gave the task to the most powerful interest group in the industry, the AMA (which had, of course, graciously offered its services). “And that was the point where I knew the system had been co-opted,” Hsiao told me. “It had become a political process, not a scientific process. And if you don’t think it’s political, you only have to look at the motivation of why AMA wants this job.”
The AMA spends at least $7 million a year running the RUC, according to its own estimates, and that includes maintaining about six full-time staff members. For that, it gets a very good return on investment. The first boon is that, in order to be on the RUC, specialty societies must become dues-paying members. At a time when the AMA has struggled against being overshadowed by specialty societies, controlling the RUC prevents what might otherwise be a rapid exodus of membership. As one RUC member told me bluntly, “No one cares about AMA. They care about the RUC.” And that’s a lucky break for the AMA. In 2012, dues collection actually increased by 3 percent, topping out at $38.6 million for the year. Cha-ching.
The second boon for the AMA is that by controlling the RUC, it controls much of the source code that our health care system uses to operate. Every single one of those roughly 9,000 medical services and procedures has its own five-digit code, known as current procedural terminology (CPT), and the AMA owns them all. That means that anyone—physicians, labs, hospitals, you name it—who wants to bill Medicare, Medicaid, or a private insurance company has to purchase either AMA books and products, or products from other software companies that pay AMA royalties and licensing fees to use the CPT codes. According to its annual report, in 2012 the AMA made $83.1 million in “royalties and credentialing products,” a large chunk of which comes from licensing CPT. Again: cha-ching.
And that’s just the monetary stuff. The third boon—the real power curve—is the fact that the AMA’s control of the RUC makes it indispensible to everyone and everything in a $2.7 trillion health care industry. That includes specialty societies, primary care organizations, and medical device and pharmaceutical companies—all of whom have something big to gain or lose from the RUC’s decisions.
The AMA cannot be unaware of this staggering power. Still, its official line about the RUC is that it’s simply doing the U.S. government a favor—offering its professional recommendations free of charge. Chaired by Dr. Barbara Levy, who is also the vice president of health policy at the American Congress of Obstetricians and Gynecologists, the RUC is simply a gathering of volunteer experts who jettison their personal interests and behave “like the Supreme Court” on behalf of the public good, according to the AMA.
But in talking to a half-dozen current and former RUC members, including both generalists and specialists, the image of the committee that emerges is less a gathering of angels, cloaked by some Rawlsian Veil of Ignorance, and more akin to a health care-themed Game of Thrones. Several RUC members I spoke to mentioned that the chairwoman often reminds the committee to “Put your RUC hat on,” meaning: “Don’t think from your society’s standpoint.” But everyone I spoke to said that specialty societies on the RUC form coalitions and alliances. Two doctors told me that “personal loyalties” play a major role in determining the way that RUC members vote. “There’s no denying it’s a highly, highly, highly politicized process,” a RUC member told me.
Here’s how the process works. Every time a new procedure comes along, a special committee at the AMA called the CPT Editorial Panel decides whether or not it needs to create a new CPT code for it. The need for a new code is sometimes tied to a new device—a valve or pump or robot that, if it is to be used, requires that doctors perform a new procedure.
Importantly, it’s not the panel’s job to weigh in on whether a new procedure is more effective or cost-efficient than a traditional method. The Food and Drug Administration has to approve a new device for the panel to consider it, but other than that the panel’s job is limited. It simply decides if a new procedure is sufficiently different from existing procedures already in the CPT; if it is, then it is assigned a CPT code, and then sent off to the RUC to be assigned a relative value unit.
 When either updating an old RVU or coming up with a new one, the RUC members spend most of their time debating something called “work units”—a slippery currency that combines how much time, training, technical skill, physical and mental effort, and stress are required of a doctor when performing a certain procedure or service. For example, according to the 2013 RUC database, “freezing off” a suspicious-looking lesion or freckle, known in the medical parlance as a “destruction,” has been assigned 1.22 work units; inserting a single-valve cardiac stent, 33.75.
When either updating an old RVU or coming up with a new one, the RUC members spend most of their time debating something called “work units”—a slippery currency that combines how much time, training, technical skill, physical and mental effort, and stress are required of a doctor when performing a certain procedure or service. For example, according to the 2013 RUC database, “freezing off” a suspicious-looking lesion or freckle, known in the medical parlance as a “destruction,” has been assigned 1.22 work units; inserting a single-valve cardiac stent, 33.75.
By many accounts, the resulting debates are often spectacularly absurd. The RUC’s database features page upon page describing what exactly a doctor does when performing each procedure. How many minutes must a doctor spend waiting for a patient to get dressed or undressed? How much time does it take to scrub in, or wait around? To read a chart? Each of these questions can bring sometimes hours of haggling at the meetings.
And then there’s the even more slippery idea of how much “mental effort” or “stress” a given procedure requires. How stressful is it to, say, perform a surgery that requires a doctor to stop a patient’s heart? And, since all of these values are relative to one another, is that level of stress greater or less than having an office visit with, say, an emotionally disturbed teenager suffering from multiple illnesses?
It’s at this point that most people—both AMA representatives and critics of it—are in agreement: at best, this is a deeply imperfect system, mired by necessity in the minutiae of doctors’ actions. But while RUC supporters argue that it’s simply the best we’ve got, critics contend that by taking an already imperfect system and handing it over to precisely those groups with the biggest material interests at stake, we’re making it even worse.
Coming up with the exact number, down to the hundredth decimal point, illustrating the “work units” for a given procedure is an admittedly thankless task. But when the RUC does it, it relies to a large degree on the testimony of—who else?—the most affected specialty society on the RUC. For instance, the American College of Cardiology will give a presentation arguing for the precise amount of time and effort required to perform a cardiac stent; the urologists weigh in on how long a catheter procedure should take. The RUC’s argument here is that the most affected specialty society knows the most about how much work, time, and stress go into the procedures its members perform.
But, of course, that specialty society also has the most to gain by inflating that value. For one, it’s in that society’s direct interest to get its members paid as much as possible. For another, the most affected specialty society often receives a good chunk of its funding from pharmaceutical and medical device companies—companies that also have a direct stake in the RUC’s proceedings. When the RUC offers up generous reimbursement rates for a specific procedure, doctors generally do it more often, and that means they use more of certain drugs and devices, too. It’s a positive feedback loop—and everyone knows it.
And then there’s the fact that much of the “data” these affected specialty societies trot out in front of the RUC would not pass the laugh test in a high school stats class. After all, these specialist societies get their data from surveys of their own membership—a group of people who stand to gain directly and materially from making a procedure seem as difficult, time-consuming, and stressful as possible. And respondents can’t exactly plead ignorance. They know darn well how the results of those polls will be used, and in case they forget, the surveys are printed with a reminder: your response is “important to you and other physicians because these values determine the rate at which Medicare and other payers reimburse for procedures,” according to a 2010 Wall Street Journal article.
What’s more, RUC rules require as few as thirty survey responses—a meager sample size, even if everyone involved weren’t both self-selected and personally invested in the results. “You wouldn’t use the results of thirty surveys to determine anything, much less billions in taxpayer cash,” a former adviser to the RUC told me.
There’s good reason to take into account the experience of those doctors who perform the procedure in question, said John Goodson, a primary care physician and associate professor at Harvard Medical School who has written about the RUC, “but if the process of assigning values to physician services is to be trusted, then the profession should hold itself to the same high, evidence-based standards that it does in other domains.”
 Another flaw in methodology comes from the fact that the RUC often relies on records from teaching hospitals in determining how long an operation takes, even though teaching hospitals often have longer surgery times than nonteaching hospitals. A 2006 study by the nonprofit health care research firm RTI International compared the amount of time the RUC suggested for sixty surgeries to data from 148 hospitals’ actual surgery logs. The RUC’s estimated times were often longer—sometimes by up to two hours.
Another flaw in methodology comes from the fact that the RUC often relies on records from teaching hospitals in determining how long an operation takes, even though teaching hospitals often have longer surgery times than nonteaching hospitals. A 2006 study by the nonprofit health care research firm RTI International compared the amount of time the RUC suggested for sixty surgeries to data from 148 hospitals’ actual surgery logs. The RUC’s estimated times were often longer—sometimes by up to two hours.
Perhaps the most damning aspect of the RUC’s methodology, however, is that, while its members often spend quite literally hours debating if a certain procedure takes three minutes or just two, the RUC never so much as flicks at the question of how much—or even whether—a procedure actually benefits patients. This failure, which is part of a broader flaw in federal health care policy, is enormously damaging to the practice of American medicine. Among other things, it means that many patients wind up undergoing expensive procedures for which more effective and less costly alternatives are available.
The AMA’s main defense against the charge that the RUC skews health care spending toward specialists’ costliest procedures is that the system is self-policing. The members are working within a fixed budget, the AMA says, so they keep each other in check: if the RUC votes to raise the RVU of one procedure, it has to account for that increase by decreasing RVUs of other procedures elsewhere. And that’s true—as far as it goes. The process does indeed involve much squabbling among specialist societies, and RUC representatives do sometimes end up voting to lower codes that would positively affect their own societies. “There’s a certain calculation that happens, and people definitely vote against themselves,” a former RUC member told me.
But this inter-society bargaining occurs in a context in which there’s already a baked-in directional bias toward increasing the value of technical procedures, which are updated regularly and constantly fine-tuned, rather than cognitive or diagnostic services, which are mostly left alone. It also occurs in a context in which one side is politically weaker than the other. The most important cleavage within the RUC is between specialist doctors, who make the bulk of their money billing for procedures, and primary care doctors, who generate most of their income from office visits. While the primary care docs make up roughly 40 percent of physicians nationwide, they have only 14 percent of the votes on the RUC. Primary care physicians now have four rotating seats on the committee—up from just two seats a few years ago—out of a total of twenty-nine voting seats. (Of the thirty-one-doctor panel, two permanent seats are nonvoting positions.) Since a vote passes with a two-thirds majority, their political clout is extremely limited.
In 2005, this baked-in two-faction system erupted into a full-blown war during a RUC meeting when the two representatives from primary care threatened to leave the committee if it did not increase compensation for office visits, according to people who were present at the time. Powerful specialty societies, who didn’t want to see the amount of the pie remaining to pay for procedures decreased, vehemently opposed the idea.
Dr. Tom Felger, a former director of the American Academy of Family Physicians who was on the RUC at the time, told me that the American College of Surgeons had even created a spreadsheet, which they shared with other surgical specialties, illustrating exactly how much the RUC could increase the value of the office-visit CPT codes without affecting surgeons’ income. “They had done the math. They knew the facts,” said Felger, who represented the AAFP at RUC meetings for a decade. “When I saw it, I thought, ‘Wow-ee, this is it—now that’s collusion.’ ”
In 2007, the RUC did finally vote to increase the RVUs for office visits, redistributing roughly $4 billion from different procedures to do so. But that was only a modest counter to the broader directionality of the RUC, which spends the vast majority of its time reviewing, updating—and often increasing—the RVUs for specific, technical procedures that make specialists the most money. Because of the direct relationship between what Medicare pays and what private insurers pay, that has the result of driving up health care spending in America—a dynamic that will continue as long as specialists dominate the committee.
And despite the RUC’s vote to increase office-visit codes, the large payment gap between primary care doctors and specialists still exists. In 2012, radiologists and orthopedists made on average nearly twice as much ($315,000) as pediatricians ($156,000), while family doctors and those specializing in diabetes and endocrinology made nearly $140,000 less than urologists. “If … a primary care doctor is making a fraction of what an orthopedist is making, then that distorts the health care system in a whole variety of different ways,” said Vladeck, the former head of the CMS under Clinton. “You really have to think about what that’s doing down the line.”
One effect is that fewer young doctors choose to go into primary care. Another is that existing primary care docs cram more and more patients into their schedules to make up cost on volume and, as a result, have only a few minutes to consult with each one (see Candice Chen, “A Day in the Life of a Primary Care Doctor,” page 42). “If you run a practice and have bills to pay—that’s going to weigh on you,” says Kavita Patel, a primary care internist at Johns Hopkins Medicine and former health care adviser at the White House. “I see twenty-eight patients in a day. I spend seven to eight minutes with a patient. That’s unrealistic—it’s crazy.”

The good news is that there’s been some incremental progress in the past few years. For example, a more empirical system is now in place for selecting the CPT codes that the RUC reviews every year. The CMS has also cracked down on certain types of redundant billing. “We’ve reduced payments for high-cost imaging quite significantly,” Jonathan Blum, the current director of the CMS, told me. “And we’ve eliminated payment codes we thought were overvalued, contrary to recommendations of the RUC.”
The CMS touts that in the last couple of years it has accepted only 60 percent of the RUC’s recommended RVUs—down from an average of about 90 percent over the past twenty years. (For technical reasons, it’s fair to say that the 60 percent number is somewhat exaggerated, but it is still a step in the right direction.)
The Affordable Care Act also takes some incremental steps toward reforming the payment system. It requires that the CMS create new “mechanisms” for establishing the physician fee schedule, which can include increasing its own in-house data collection and analysis to correct, corroborate, or refute the RUC’s recommendations, especially for inputs that are more easily measured empirically, like determining how long on average a given surgery takes. To comply, the CMS recently commissioned two reports from the RAND Corporation and the Urban Institute to advise the agency on how best to do that.
The CMS, in cooperation with the AMA, is also considering rolling out new codes that may make it easier for primary care doctors to bill for services for which they weren’t previously compensated. This year, for example, they introduced two so-called transitional care management (TCM) codes that will allow doctors to bill Medicare for the time they spend helping patients transition from an in-patient setting to another community or their homes.
Yet while some of these incremental changes have been supported by the AMA and the powerful specialty societies (which, indeed, have nothing to lose from, say, TCM codes), other attempts at reform have been met with fierce push back—from organized letter campaigns to intense lobbying—and it is not clear if they will survive.
“CMS is in a no-win situation,” says Vladeck. “They’ve got extremely powerful forces making extraordinary amounts of money, and if CMS tries to change that, it’s really easy for the providers to say, ‘This is going to impair access,’ or ‘This is going to hamper care,’ even if there’s zero reality to that claim. People like doctors and nurses, and they don’t like government bureaucrats.”
Even if these incremental steps remain in place, some critics argue they are akin to frosting on a rotten cake. “You can make these tweaks,” says Brian Klepper, a health care analyst and principal at WeCare, a primary care clinic and medical management firm, “but what you’re doing is ignoring the fact that this system is fundamentally insane. It’s so corrupt and collusive, it’s not something that can be incrementally fixed.”
Long term, there are two basic options to really solving the problems caused by the RUC. The first is to take the process away from the control of the AMA and put it in the hands of a well-resourced group of experts under the auspices of the federal government. This might take the form of a panel of doctors employed by the government, or of an advisory committee of representatives of different medical societies but with greater representation of primary care doctors. While the latter set-up would hardly eliminate all conflicts of interest and political horse trading, such a committee would at least have to meet federal requirements for disclosure of all conflicts of interest. It would also be required to publish minutes from the meetings, data from any surveys used, and so forth. That would be a big improvement over the current, closed-door policy at the RUC, which, because it’s convened by a private entity, the AMA, enjoys First Amendment freedom from federal disclosure rules.
This option, however, is politically tricky. “The AMA and these medical specialty societies have power, and they’re not wild about seeing that power diluted,” said Zeke Emanuel, a former special adviser on health policy to the Office of Management and Budget and the National Economic Council, and an oncologist. “So yeah, if you ask the sober policy community, ‘Should we do this?’ their opinion is yes. But when it comes to this, the sober policy community has almost never held sway.”
In 2011, Washington Democratic Congressman Jim McDermott proposed a bill that would have furnished the CMS with resources to assemble an independent council of advisers. It was met with a strongly worded letter from the American College of Surgeons the day it was proposed and died in committee that afternoon.
Some reformers point to a provision in Obamacare that might allow for an end run around Congress. The law creates a new entity, the Independent Payment Advisory Board, which, if Medicare costs outstrip the Consumer Price Index, will have the power to cut or change Medicare provider payments unilaterally. Its decisions can be overturned by Congress only if lawmakers pass alternative cost-cutting measures of equal size. Statutorily, IPAB could create a government-run equivalent of the RUC. Whether it will ever get a chance to exercise that power, however, is an open question: IPAB is a major political target for both Republicans who are demanding its immediate abolition and some Democrats who enjoy close ties to the medical drug and device industry.
The second option to solving the RUC problem would be to get Medicare out of the business of funding fee-for-service medicine. Reformers have been complaining for years that paying providers per procedure creates incentives for gaming and overuse that are difficult, if not impossible, to overcome. Under Obamacare, the CMS is already taking modest steps away from fee-for-service billing by expanding experiments in “bundled payments,” whereby providers are paid a lump sum to take care of patients with certain conditions, like diabetes or heart disease. The AMA, aware of the growing backlash in Washington against fee-for-service, has endorsed some of Medicare’s bundling initiatives.
But we need to go much further. It’s no coincidence that numerous studies have found that the best-quality and lowest-cost health care in America can be found in systems like Veterans Affairs and Utah’s Intermountain Healthcare where doctors are on salary and paid for keeping their patients well, not according to a fee-for-service system. As this magazine has argued (see Phillip Longman, “The Cure”), the federal government should set a certain date at which Medicare will pay only for health services provided by integrated systems.
Such a move would be fiercely resisted by organized medicine, and specialist societies in particular. But it would be the surest way to control the nation’s health care costs while improving health outcomes. And it would have a delightful side benefit: with fee-for-service eliminated, there would be no need to have thirty-one doctors sit in a ballroom in Chicago and centrally plan the pricing minutia of thousands of medical services and procedures. The RUC, in other words, would be made obsolete.
Haley Sweetland Edwards is an editor of the Washington Monthly.
Article link: https://washingtonmonthly.com/magazine/julyaugust-2013/special-deal/#.WkPNfAfnnEp.twitter

More and more companies are realizing they must reinvent their cultures by infusing innovation into their DNA. Unlike startups that get to shape culture from scratch, established companies must transform existing norms, values, and assumptions in ways that inspire everyone to innovate — not just at the top of the organization, but at all levels.
One company that’s making headway on that goal is CSAA Insurance Group (CSAA IG), one of the insurance companies affiliated with the 55 million-member American Automobile Association (AAA). With almost 4,000 employees, CSAA IG has embarked on a systemic approach to create a pervasive culture of innovation. The tactics being used by CSAA IG are all ones that leaders in other companies can apply to their own innovation culture change efforts.
Early on, CSAA IG’s executive team recognized that to create a culture of innovation, the organization needed to do more than embrace individual innovation projects. To ensure a truly transformative culture change effort, the team outlined a new corporate-wide organizational strategy to sit alongside its other market-focused strategies: “Foster a culture of insight and innovation.” They also made it part of their talent management approach: Innovation was added to the company’s values statement and included as a core competency to consider in assessing, rewarding, and developing employees.
But they also realized that the term “innovation” was pretty vague; if they were measuring people on it, and making it part of their strategy, they’d have to be more concrete about what they meant by it. CSAA IG’s executive team outlined three specific types of innovation — incremental, evolutionary, and disruptive — to help employees understand their roles in fostering a culture of innovation.
Most people focus on the first type of innovation: incremental. Leadership realistically expects that the vast majority of the company’s innovation will involve smaller tweaks that advance the core business. It’s perfectly OK that most people – from call center employees to claims adjusters in the field – focus on continuous improvements to current business processes, the customer experience, and insurance products.
While the company also wants “evolutionary” (e.g., creating new digital customer experiences) and “disruptive innovation” (e.g., exploring the insurance implications of self-driving cars) as part of its innovation strategy, fewer overall resources are allotted to these larger efforts. It’s all part of CSAA IG’s portfolio approach.
To help employees spot these opportunities, CSAA IG delivers innovation training to all employees. Its program provides tools and applied exercises based on design thinking, and makes it clear that everyone can—and should—contribute creative ideas for improvement in business processes, customer experiences, and product offerings. Employees participate in a half-day program that tackles real business problems facing their workgroups, and results in a prioritized list of ideas.
This all-hands-on-deck approach to innovation training has not only provided a greater sense of ownership and engagement among CSAA Insurance Group’s workforce, it has produced tangible results. For example, a team of insurance underwriters analyzed call data and led improvements to voice prompts that reduced misrouted phone interactions to their department by 40 percent. Other teams have helped streamline the process for issuing proof of insurance cards and are contributing to prototyping efforts for “smart claims” systems, allowing customers to submit images of damaged property for online assessment.
There’s nothing worse for a company’s innovation culture than soliciting ideas and doing nothing with them. So to ensure that employees’ ideas actually get implemented, CSAA IG’s managers are expected to engage their teams after the training sessions to select specific ideas to implement based on what everyone just generated. Employees also have access to CSAA IG’s “Innovation Hub,” an online portal, that includes a self-service smorgasbord of resources including a design thinking toolkit, calendar of innovation-related events, self-paced training materials, articles from innovation experts, and more. The company also set up an idea management platform, where various departments can post their innovation challenges, and where the crowd can contribute, evaluate, and develop solutions.
To help generate excitement for the idea management platform, during the first online innovation challenge event, anyone who submitted an idea was surprised with a physical paper light bulb posted in their cubicle workspace. With light bulbs popping up all around the office, employees’ motivation to participate skyrocketed – and the company’s first online challenge received an 80% participation rate.
Creating a culture of innovation is about much more than hiring a Chief Innovation Officer or creating a new department. Culture change takes time and significant effort, and shifting culture toward innovation is no different. The process may start at the top, but it’s fundamentally about getting all employees involved.
Article link: https://hbr.org/2017/08/how-one-insurance-firm-learned-to-create-an-innovation-culture

Soren Kaplan is an Affiliated Professor at the Center for Effective Organizations at USC’s Marshall School of Business. He is the author of The Invisible Advantage and founder of InnovationPoint.
