Report link:
https://healthcarereimagined.net/wp-content/uploads/2019/05/dib_5g_study_04.04.19.pdf
Written by Tajha Chappellet-Lanier
Apr 5, 2019 | FEDSCOOP

While the rollout of 5G wireless capability will be driven by private industry, its emergence has big implications for the Department of Defense, a study by the Defense Innovation Board warns.
The debut of 5G will present many opportunities for the DOD, the DIB says in a new report. It will enable higher capacity for data transfer, increased efficiency, new technologies like hypersonic weapons and more. But it also poses some security risks.
The DIB, an advisory board of tech industry leaders first introduced in 2016, released the unclassified version of this report — co-written by vice president of wireless at Google, Milo Medin, and tech venture capitalist Gilman Louie — Thursday.
The report details the current state of global 5G competition and what the technology will mean for DOD operations. It also includes some recommendations on how the defense agency should proceed. Per its charter, the DIB cannot force DOD to adopt any strategies, but it does make suggestions the agency may choose to follow.
“The shift from 4G to 5G will drastically impact the future of global communication networks and fundamentally change the environment in which DoD operates,” the recent report states. As with past developments, it goes on, there will be a first-mover advantage. And at the moment, China is poised to be that first mover.
“China is on a track to repeat in 5G what happened with the United States in 4G,” the report states.
China’s lead is owing to investment, yes, but the other issue is the lack of spectrum. 5G will require more spectrum availability, and there are two approaches that countries are taking to this. One involves the electromagnetic spectrum below 6 GHz — this is called “sub-6.” The other approach clues in on the part of the spectrum between about 24 and 300 GHz and this is called “mmWave.” China’s efforts are focused on sub-6 while the U.S. is focused on mmWave. Both have benefits and challenges — “the future of 5G may involve some combination of both,” the report states.
However, the report argues, if China moves first with sub-6 and other nations follow that lead, the U.S. might find itself faced with interoperability challenges, not to mention security risks.
“As sub-6 becomes the global standard, it is likely that China, the current leader in that space, will lead the charge,” the report reads. “This would create security risks for DoD operations overseas that rely on networks with Chinese components in the supply chain. Even if the United States were to restrict use of Chinese equipment suppliers domestically, the United States is not a big enough market in wireless to prevent China’s 5G suppliers from continuing to increase market share globally, resulting in significant pressure on a declining set of vendors that would serve the U.S. market.”
The report concludes by suggesting that the DOD “make a plan for sharing sub-6 GHz spectrum,” “prepare to operate in a ‘post-Western’ wireless ecosystem” by adopting a zero-trust network model and advocate for trade policies that serve to secure the supply chain. A fourth recommendation is classified.
Article link: https://www.fedscoop.com/defense-innovation-board-5g-report-dod/
-In this Story-
5G, 5G network, China, Defense Innovation Board, Department of Defense (DOD), wireless spectrum

The high cost of gene and cell therapies will make it critical for companies to provide higher levels of support for healthcare providers and especially for patients through access, reimbursement, and financing.
The new generation of rapidly emerging gene and cell therapy companies are advancing many promising and potentially curative treatments for major areas of unmet need in healthcare. They are poised to transform the biopharmaceutical industry in the years ahead. A recent report from the Pharmaceutical Research and Manufacturers of America (PhRMA) shows there are nearly 300 novel gene and cell therapies currently in clinical stage development around the world for treatment of a wide range of diseases and conditions, with the majority in oncology.
Some of the most advanced products are being developed by a small number of larger pharmaceutical companies and by innovative small biotechs. In many cases, companies either have, or are building, the range of expertise and resources necessary to advance their products to commercialization. For others, it is essential to consider the full range of options to bring their products to patients and choose the path that will maximize both commercial interests and patient access.
In light of the many risks inherent in “going it alone,” many industry insiders expect to see more M&A deals between small gene and cell therapy companies with late-stage assets and larger entities positioned to handle global commercialization. When assessing their options, there are several factors smaller life sciences companies should consider, including the level of financing required and access to capital to support a commercialization strategy, availability of skilled workers to handle complex manufacturing and distribution processes, the potential need for new levels of innovation and flexibility in pricing models and access strategies, and the need for significant investment in patient and clinician education, monitoring, and support.
Manufacturing and supply chain complexity
Among the challenges in development of gene and cell therapies, access to technology is a primary consideration. Alignment with larger companies can provide smaller biotechs access to manufacturing and distribution capabilities that may be out of reach. Conversely, larger companies often seek to acquire innovative development programs to build their pipelines but also expand their R&D capabilities through the acquisition of relevant new platform technologies in the field.
Gene and cell therapy companies are distinct from more traditional drug development programs including small molecules and monoclonal antibodies in that some risks are more significant at later stages of development. In many cases, the final mode of drug delivery for a gene therapy cannot be determined until late in the development program. At the commercial stage, efforts to scale up production to meet demand can also put stress on both manufacturing and distribution protocols.
Efforts to confirm an optimal drug delivery platform and execute production at a large scale require very specialized expertise and advanced manufacturing and supply chain management capabilities that are not readily available to smaller companies. Success will depend on access and optimal use of innovative technologies including advanced cryopreservation tools.
Companies must continually assess their ability to invest in the right technology at the best time – too early and it can squeeze resources needed for other projects, too late and it can affect scale-up when needed. The distribution chain for gene and cell therapies must also reflect the fact that most products have a very short half-life (often days) and require carefully controlled transport conditions.
Sales and marketing
Gene and cell therapies will also require new strategies in sales and marketing to support commercialization. While some shifts are beginning to occur, today’s go-to-market models are still mainly relying on an extensive sales force and large marketing and advertising budgets.
But this approach is not suited to gene and cell therapies, especially potentially curative therapies administered in a single dose and targeting very small patient populations in rare diseases. New approaches will require more targeted medical and scientific communications with clinicians but also patients, and other stakeholders, and more precise targeting of patients and healthcare providers.
It will be essential for companies to use predictive analytics to define appropriate patient cohorts and data analyses of diagnoses and procedures to map the patient journey and identify an effective marketing strategy. Companies should be prepared to support sales with a few experts including medical science liaisons rather than a large sales force. These experts will play a vital role in clinician and patient education. In fact, many industry insiders anticipate that a traditional sales force could become obsolete in marketing for gene and cell therapies.
New pricing models
Gene and cell therapies are often priced high due to factors including complex production processes, potentially curative efficacy, and the fact that they are designed to treat rare diseases with small patient populations for which there are few, if any, options.
The first approved gene therapy, Glybera, a treatment for patients with the rare lipoprotein lipase deficiency, was priced at $1 million after it was approved. While costs may reflect the benefits that these therapies bring to patients and health systems over time, significant different models may be needed to support payment for the one-time application of a curative therapy. These innovative models include value-based pricing, annuity payments, and expanded risk pools. Many gene and cell therapies also will require payers and clinicians to make decisions related to access and treatment without the levels of long-term efficacy and safety data typically available to support new drugs.
With respect to payment options, value-based agreements require that products meet specific and timed clinical targets to be eligible for reimbursement from payers. This can reduce the risk of coverage for unsuccessful treatments and help address the issue of limited evidence of efficacy and safety at launch. All relevant stakeholders, however, will need to align on what constitutes a successful treatment outcome within a pre-defined time period.
The annuity payment model is another option to pay for the significant long-term benefits of gene and cell therapies. With this approach, payers would agree to coverage based on a series of payments over a set timeline for each patient treated with a curative therapy. This could reduce the near-term budget impact for payers while accounting for longer-term value. As with value-based agreements, annuity payment models would require stakeholders to agree on what constitutes a successful outcome and centralize outcomes data management and reporting, which in itself is a considerable challenge.
Alternatively, to expand risk pools, commercial payers could join with other stakeholders, potentially including government and nonprofits, to help keep premiums and cost sharing at manageable levels. But many payers anticipate that expanded risk-sharing models will face challenges in achieving the necessary levels of broad alignment to be viable.
The high cost of gene and cell therapies will make it critical for companies to provide higher levels of support for healthcare providers and especially for patients through access, reimbursement, and financing. Providing a dedicated access and finance manager who is empowered to support patients will be essential. Some of this type of support is offered today for high priced oncology drugs, and helps patients understand their insurance coverage and additional financial support options, such as foundation support.
Conclusion
While the gene and cell therapy sector is trending toward more M&As, many emerging companies might choose to commercialize gene and cell therapies themselves. Success will be based on their ability to refine their go-to-market models, geographic strategies, and maximize efficiency.
Optimal strategies will include acquiring high-value manufacturing processes and technologies at the right time, building a team of specialized experts – which may involve collaboration with and support from key stakeholders – and adopting flexible and innovative pricing models to support treatment. Drug developers will also need to adjust their sales strategies to target a small, specialized audience. While the road to commercialization will include many bumps, efforts to understand and address the unique issues presented by gene and cell therapies can help many companies to find a path forward.
Article link: https://medcitynews.com/2019/01/looking-ahead-commercialization-strategies-for-gene-and-cell-therapy-companies/
Photo: Getty Images
Pascale Diesel
Pascale Diesel is Vice President in CRA’s Life Sciences Practice. Dr. Diesel has 18 years of pharmaceutical and biotech experience in global development, marketing, planning, and business development and more than 10 years of strategic consulting experience focusing on portfolio optimization and valuation. Prior to joining CRA, she was Principal, Strategy and Portfolio Analysis, EMEA at QuintilesIMS (now IQVIA), concentrating on commercial due diligence (sell- and buy-side), sustainable growth and geographic expansion. The views expressed herein are the author’s and not those of Charles River Associates (CRA) or any of the organizations with which the author is affiliated.


April 05, 2019 – The U.S. Air Force (USAF) is updating the health IT infrastructure at its military treatment facilities to prepare for MHS GENESIS EHR system implementation because of problems with a pilot deployment at Fairchild Air Force Base in Washington.
As a result of lessons learned at Fairchild, the Air Force is investing in network upgrades at least six months prior to training and go-live to alleviate technical problems experienced during the pilot MHS GENESIS implementation there, Lt. Gen. Dorothy Hogg, the Air Force surgeon general, told the Senate Appropriations Committee’s defense subcommittee on April 3.
The Fairchild pilot was one of four that the Department of Defense carried out at military facilities in the Pacific Northwest.
DoD to Roll Out Next Phase of EHR Modernization This Fall
DoD Restructures Management of Medical Treatment Facilities
DoD Health Data Exchange Gets Bridge Contract As GAO Hears Appeal
MHS GENESIS implementation “requires broad systems and network improvements, as well as business process changes to achieve standardization and culture change,” Hogg asserted in prepared testimony.
In addition, the Fairchild pilot identified issues with the USAF training program for the new EHR system. “Immature workflows limited training effectiveness for the entire staff, beyond the designated MHS GENESIS ‘super-users’ who were tasked to help other members learn the system. We developed a new training approach in coordination with the Defense Health Agency, informed by the challenges and solutions from Fairchild and the other early sites,” she related.
MHS GENESIS replaces legacy DoD EHR systems, including the Armed Forces Health Longitudinal Technology Application, the Composite Health Care System, and components of the Theater Medical Information Program-Joint.
It will support more than 9.5 million DoD beneficiaries and approximately 205,000 military health system personnel.
All DoD and VA Medical Data Will Stored in Single Database
Stacy Cummings, former program executive officer for the defense healthcare management systems, told the subcommittee that both DoD and the Department of Veterans Affairs (VA) will be using the same Cerner commercial software solution for their EHR systems and will deploy one single instance; all the medical data from the DoD and VA will be stored in a single database.
The MHS GENESIS pilot program, according to Cummings, produced the following improvements: 32 percent increase with the number of patients seen in outpatient care settings; 8.1 percent improvement in turnaround time for chemistry lab tests; 88.5 percent average in discharge medication reconciliation compliance; 84 percent average bar code medication administration compliance; and 63 percent increase in new prescriptions and refills.
Cummings, who is currently the principal deputy assistant secretary of defense for acquisition, said that the MHS GENESIS deployment will occur by region—three in the continental United States and two overseas—in a total of 23 waves. Each wave will include an average of three hospitals and 15 physical locations and will last approximately one year.
This approach allows the DoD to use lessons learned and experience from prior waves to maximize efficiencies in subsequent waves. Full operational capability, including garrison medical and dental facilities, is expected for 2023, she said in her prepared statement.
Cummings related that DoD and VA signed a joint commitment statement in September of last year, pledging to align VA and DoD strategies on deploying an interoperable EHR system. The DoD and VA then evaluated their program elements, including infrastructure, incorporating of clinical and business processes, and other requirements from the functional, technical, and programmatic communities.
To accomplish this integration, the two agencies set up the Federal Electronic Health Record Modernization Program Office, which will provide a “more comprehensive, agile, and coordinated management authority to execute requirements necessary for a single, seamless integrated EHR,” she explained.
The U.S. Coast Guard has joined the EHR implementation as well. The combined DoD-VA-USCG EHR solution will focus on clinical services, interfaces, and a shared infrastructure to enable shared workflows, user roles, order sets, training, and cybersecurity standards, Cummings concluded.
Article link: https://hitinfrastructure.com/news/ehr-pilot-issues-spur-usaf-spending-on-health-it-infrastructure


 The ceaseless battle over the 2010 law has made it difficult to address the high cost of American health care.
The ceaseless battle over the 2010 law has made it difficult to address the high cost of American health care.
By JOANNE KENEN
The Obamacare wars have ignored what really drives American anxiety about health care: Medical costs are decimating family budgets and turning the U.S. health system into a runaway $3.7 trillion behemoth.
Poll after poll shows that cost is the number one issue in health care for American voters, but to a large extent, both parties are still mired in partisan battles over other aspects of Obamacare – most notably how to protect people with pre-existing conditions and how to make insurance more affordable, particularly for people who buy coverage on their own.
That leaves American health care consumers with high premiums, big deductibles and skyrocketing out-of-pocket costs for drugs and other services. Neither party has a long-term solution — and the renewed fight over Obamacare that burst out over the past 10 days has made compromise even more elusive.
Democrats want to improve the 2010 health law, with more subsidies that shift costs to the taxpayer. Republicans are creating lower-cost alternatives to Obamacare, which means shifting costs to older and sicker people.
Neither approach gets at the underlying problem — reducing costs for both ordinary people and the health care burden on the overall U.S. economy.
Senate HELP Committee chair Lamar Alexander, the retiring Tennessee Republican with a reputation for deal-making, has reached out to think tanks and health care professionals in an attempt to refocus the debate, saying the interminable fights about the Affordable Care Act have “put the spotlight in the wrong place.”
“The hard truth is that we will never get the cost of health insurance down until we get the cost of health care down,” Alexander wrote, soliciting advice for a comprehensive effort on costs he wants to start by summer.
But given the partisanship around health care — and the fact there have been so many similar outreaches over the years for ideas, white papers and commissions — it’s hard to detect momentum. Truly figuring how to fix anything as vast, complex and politically charged as health care is difficult. Any serious effort will create winners and losers, some of whom are well-protected by powerful K Street lobbies.
And the health care spending conversation itself gets muddled. People’s actual health care bills aren’t always top of mind in Washington.
“Congress is looking at federal budgets. Experts are looking at national health spending and the GDP and value. And the American people look at their own out-of-pocket health care costs and the impact it has on family budgets,” said Drew Altman, the president and CEO of the Kaiser Family Foundation, which extensively tracks public attitudes on health.
But Congress tends to tinker around the edges — and feud over Obamacare.
“We’re doing nothing. Nothing. We’re heading toward the waterfall,” said former CBO director Doug Elmendorf, now the dean of the Harvard Kennedy School, who sees the political warfare over the ACA as a “lost decade,” given the high stakes for the nation’s economic health.
The solutions championed by the experts — a mix of pricing policies, addressing America’s changing demographics, delivering care more efficiently, creating the right incentives for people to use the right care and the smarter use of high-cost new technologies — are different than what the public would prescribe. The most recent POLITICO-Harvard T.H. Chan School of Public Health poll found the public basically wants lower prices, but not a lot of changes to how — or how much — they consume health care, other than spending more on prevention.
Lawmakers are looking at how to start chipping away at high drug prices, or fix “surprise” medical bills that hit insured people who end up with an out-of-network doctor even when they’re at an in-network hospital. Neither effort is insignificant, and both are bipartisan. While those steps would help lower Americans’ medical bills, health economists say they won’t do enough to reverse the overall spending trajectory.
Drug costs and surprise bills, which patients have to pay directly, “have been a way the public glimpses true health care costs,” said Melinda Buntin, chair of the Department of Health Policy at Vanderbilt University School of Medicine. “That information about how high these bills and these charges can be has raised awareness of health care costs — but it has people focused only on that part of the solution.”
And given that President Donald Trump has put Obamacare back in the headlines, the health law will keep sucking up an outsized share of Washington’s oxygen until and quite likely beyond the 2020 elections.
Just in the last week, the Justice Department urged the courts to throw out Obamacare entirely, two courts separately tossed key administration policies on Medicaid and small business health plans, and Trump himself declared he wants the GOP to be the “party of health care.” Facing renewed political pressure over the party’s missing Obamacare replacement plan, Trump last week promised Republicans would devise a grand plan to fix it. He backtracked days later and said it would be part of his second-term agenda.
Democrats say Trump’s ongoing assaults on the ACA makes it harder to address the big picture questions of cost, value and quality. “That’s unfortunately our state of play right now,” said Rep. Raul Ruiz (D-Calif.). “Basic health care needs are being attacked and threatened to be taken away, so we have to defend that.”
The ACA isn’t exactly popular; more than half the country now has a favorable view of it, but it’s still divisive. But for Republicans and Democrats alike, the new POLITICO-Harvard poll found the focus was squarely on health care prices — the cost of drugs, insurance, hospitals and doctors, in that order.
The Republicans’ big ideas have been to encourage less expensive health insurance plans, which are cheaper because they don’t include the comprehensive benefits under Obamacare. That may or may not be a good idea for the young and healthy, but it undoubtedly shifts the costs to the older and sicker. The GOP has also supported spending hundreds of millions less each year on Medicaid, which serves low-income people — but if the federal government pays less, state governments, hospitals and families will pay more.
Last week, courts blocked rules in two states that required many Medicaid enrollees to work in order to keep their health benefits, and also nixed Trump’s expansion of association health plans, which let trade groups and businesses offer coverage that doesn’t include all the benefits required under the ACA.
House Democrats last week introduced a package of bills that would boost subsidies in the Obamacare markets and extend that financial assistance to more middle-class people. The legislation would also help states stabilize their insurance markets — something that the Trump administration has also helped some states do through programs backstopping health insurers’ large costs.
These ideas may also bring down some people’s out-of-pocket costs, which indirectly lets taxpayers pick up the tab. These steps aren’t meaningless — more people would be covered and stronger Obamacare markets would stabilize premiums — but they aren’t an overall fix.
The progressive wing of the Democratic party backs “Medicare for All,” a brand new health care system that would cover everyone for free, including long-term care for elderly or disabled people. Backers say that the administrative simplicity, fairness, and elimination of the private for-profit insurance industry would pay for much of it.
The idea has moved rapidly from pipe dream to mainstream, but big questions remain even among some sympathetic Democrats about financing and some of the economic assumptions, including about how much of a role private insurance plays in Medicare today, and how much Medicare puts some of its costs onto other payers. Already a political stretch, the idea would face a lot more economic vetting, too.
The experts, as well as a smattering of politicians, define the health cost crisis more broadly: what the country spends. Health care inflation has moderated in recent years; backers of the Affordable Care Act say the law has contributed to that. But health spending is still growing faster than the overall economy. CMS actuaries said this winter that if current trends continue, national health expenditures would approach nearly $6 trillion by 2027 — and health care’s share of GDP would go from 17.9 percent in 2017 to 19.4 percent by 2027. There aren’t a lot of health economists who’d call that sustainable.
And ironically, the big fixes favored by the health policy experts — the ones that Alexander is collecting but most politicians are ignoring — might address many of the problems that keep aggravating U.S. politics. If there were rational prices that reflected the actual value of care provided for specific episodes of illness and treatment, instead of the fragmented system that largely pays for each service provided to patients, then no medical bill would be a surprise, noted Mark McClellan, who was both FDA and CMS chief under the President George W. Bush and now runs the Duke-Margolis Center for Health Policy.
“But taking those steps take time and will be challenging,” McClellan noted. “And they’ll be resisted by a lot of entrenched forces.”
Alice Miranda Ollstein and Adam Cancryn contributed reporting.
Article link: https://www.politico.com/story/2019/04/03/obamacare-health-care-crisis-1314382
 Foreign Policy illustration
Foreign Policy illustrationThere’s no single explanation that accounts for Huawei’s success or recent technical prowess. A cost advantage helped, of course. So did state backing, government protection from foreign competitors, and a huge local market, which led to massive and swiftly multiplying revenues. And it could hardly have been mere coincidence that Huawei’s founder, Ren, was a PLA veteran, and Huawei’s first customer proved to be the People’s Liberation Army.
With a Chinese company building the network through which huge volumes of data—phone calls, emails, and business transactions—will flow across the globe, U.S. officials fear that infrastructure could be subverted for espionage, allowing Beijing’s intelligence agencies to gather huge volumes of communications.
Experts are also still debating whether Huawei is as dominant as some officials in Washington fear. Some telecoms executives with experience operating Huawei alongside equipment made by other manufacturers say that it has established the lead, especially in the bread-and-butter technology of transmitting large amounts of data through radio networks.
Article link: https://foreignpolicy.com/2019/04/03/the-improbable-rise-of-huawei-5g-global-network-china/amp/

By Martin Checinski, Roland Dillon, Solveigh Hieronimus, and Julia Klier
It is no easy matter to bring about major change in a large, complex organization—whichever sector it’s in. McKinsey research has found that 74 percent of private-sector transformation efforts fail to meet their objectives, while in the public sector, the failure rate is even higher, at 80 percent. In both sectors, people practices are a decisive factor, often making the difference between success and disappointment. Indeed, the five key success factors for government transformations all have a strong people component (Exhibit 1).
Exhibit 1
 Rachna Gandhi, a former business executive who went on to lead the Australian government agency Service NSW, put it this way: “Transformations in government are not harder than in the private sector. There are certain unique factors in both, but the toughness factor is pretty similar. Both need to emphasize bringing people on the journey and creating an emotional investment.”
Rachna Gandhi, a former business executive who went on to lead the Australian government agency Service NSW, put it this way: “Transformations in government are not harder than in the private sector. There are certain unique factors in both, but the toughness factor is pretty similar. Both need to emphasize bringing people on the journey and creating an emotional investment.”
Paradoxically, the importance of people practices in transformations is both good and bad news for public-sector change leaders. On the one hand, governments’ public-service mission gives them a distinct advantage over private-sector peers when it comes to mobilizing people to live their values and achieve social outcomes. On the other, there is a lot of evidence that structures and cultures in government make them more change resistant than business organizations, reducing their overall organizational health and effectiveness.
How should government leaders think about people-driven change? McKinsey research—along with the insights of successful transformation leaders—points to three essential practices:
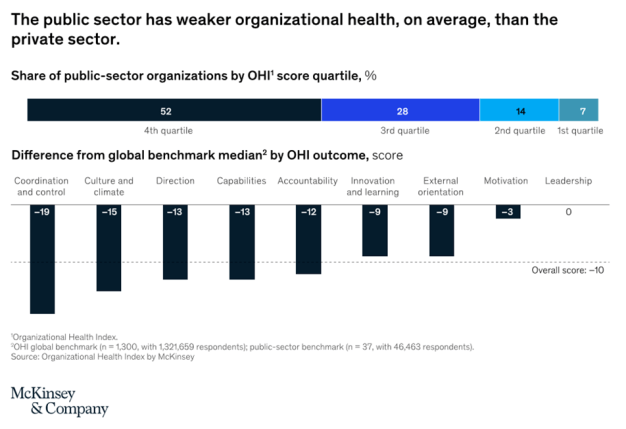
Organizations can measure and manage health—in other words, how well they align, execute, and renew—with the same rigor as they manage performance. McKinsey has measured the health of over 2,000 organizations in both the public and private sectors through our Organizational Health Index Survey, which to date has had over five million respondents. This research indicates that over 75 percent of public-sector organizations have below-average health. Moreover, the research makes it clear that gaps in organizational health in the public sector are particularly apparent in culture, coordination, and capabilities (Exhibit 2). Only in the dimension of leadership do public-sector organizations match the health of their private-sector peers.
Exhibit 2
 In addition to disadvantages in organizational health, public-sector institutions face a series of complex people-related challenges that their private-sector counterparts have to navigate to a lesser degree. This makes their starting points and journeys quite different when it comes to engaging employees and building capabilities during transformation efforts.
In addition to disadvantages in organizational health, public-sector institutions face a series of complex people-related challenges that their private-sector counterparts have to navigate to a lesser degree. This makes their starting points and journeys quite different when it comes to engaging employees and building capabilities during transformation efforts.
First, public-sector organizations typically have more risk-averse cultures than private-sector businesses, where employees who innovate are often richly rewarded. That’s no surprise, given a risk environment in the public sector that can only be described as asymmetric: civil servants are more likely to be penalized for failure than they are to be rewarded for innovation or outperformance. For example, a bold experiment that improves a service for the majority of recipients is unlikely to win kudos for the responsible civil servants if a small number of vocal citizens complain about the change. Likewise, a public-sector manager who succeeds in improving efficiency in his or her department might be “rewarded” with a reduced budget—but punished with a poor performance review if the effort fails.
Understandably, many civil servants view ambitious change programs with extreme caution. To break through this risk aversion, public-sector leaders must work consciously to shift the organizational culture, giving senior civil servants clear mandates for change and strong performance measures tied to improved outcomes. They can also take a leaf out of the book of business leaders who celebrate failure among their employees as a necessary by-product of innovation.
A second challenge for public-sector change leaders is the limitations of political mandates. Public-sector change efforts may be held back by the extent of the government’s political mandate, which may be weak or short lived, owing to the frequency of elections. A related challenge is that public-sector leaders typically have shorter tenure than their private-sector counterparts. For example, a review of ministers of health across 23 countries from 1990 to 2009 found that half of them left office in under two years. The tenure of senior civil servants is falling too: in the United Kingdom, for example, annual churn in the cabinet office rose from 20 percent in 2010 to 35 percent in 2016. By contrast, the average tenure of CEOs of major US companies is around eight years.
In these circumstances, successful public-sector transformations require laser-like focus from leaders. McKinsey’s research shows that efforts that are focused on a small set of true priorities are much more likely to succeed than initiatives that attempt to change everything at once. Moreover, frequent turnover at the top means that successful public-sector transformations must be anchored in frontline staff—the people who continue running the organization when the leader moves on. This was the approach taken by Service NSW. The agency aimed to simplify citizen access to government services, with a shift to digital transactions and a “one-stop-shop” approach to improve customer experience. It rooted its initiatives in frontline staff, who were empowered to develop and implement improvement ideas. Because the agency’s initiatives were owned by the people who were actually going to run them, they were hugely successful: Service NSW achieved customer-satisfaction rates of 97 percent.
The third challenge is that many major change efforts must work across multiple government departments or agencies, as new-generation solutions do not usually fit neatly within existing portfolios. Each institution involved in a transformation is likely to have distinct strengths and gaps in capabilities and frequently conflicting motivations. The implication for change leaders is that they must invest time and energy in building support and collaboration from people they do not directly influence.
Whereas a private-sector CEO leading a change effort will usually have the majority of people involved within their own organization, a minister or head of department in government will need to work with several other ministers or departments. For example, an effort to improve tourism outcomes will require collaboration between the ministry of tourism and those of transport, economic development, foreign affairs, and so on—as well as with city mayors and the private sector. Indeed, McKinsey’s research finds that 70 percent of public-sector transformation efforts were scoped across more than one ministry, department, or agency.
Any government leader embarking on a major change effort must face these challenges head on—and take deliberate steps to mitigate them. Yet the public sector also has distinct advantages vis-à-vis the private sector. In particular, public-sector organizations are in a unique position to tap into talent from the broader society. For example, when Germany’s government grappled with the influx of hundreds of thousands of refugees in 2015, it was able to mobilize massive involvement from citizens and civil-society organizations. An estimated one in ten adults in Germany was involved in voluntary refugee assistance in the summer of 2015.
In India, the state of Maharashtra invited college students to come up with ideas to solve 11 critical challenges, ranging from eradicating drought to using technology to expedite justice. The Transform Maharashtra competition attracted more than 11,000 student participants. Not only do such initiatives “crowd in” ideas and capabilities from beyond the civil service, they also enable governments to drive change with fewer public resources than would otherwise be needed.
The successful transformations we studied were steered and championed by deeply committed leaders. Each of them devoted considerable time and energy to the effort, took personal accountability for success or failure, was a visible role model for the change, and had the courage to challenge long-established assumptions and conventions. Such leaders live and breathe the journey and stretch their capacity for strategic planning, emotional resilience, and inspiring people leadership. They also take personal responsibility for the change. An example is Mike Bush, New Zealand’s police commissioner, who led the transformation of the country’s police services to a prevention-focused model. He told us, “You need to dedicate at least 60 percent of your time inside the organization to driving a transformation.”
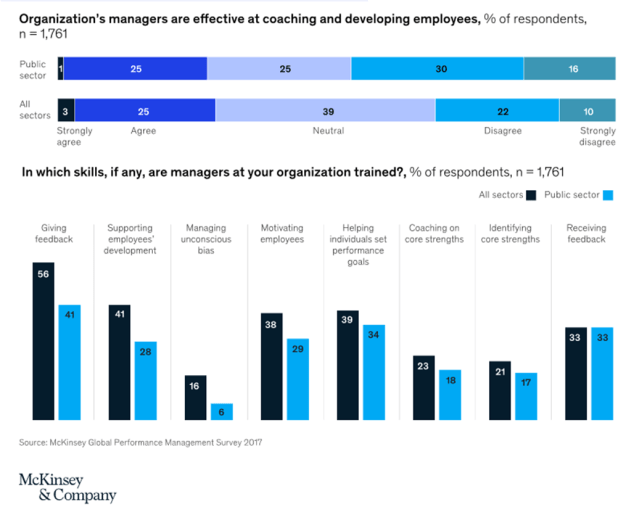
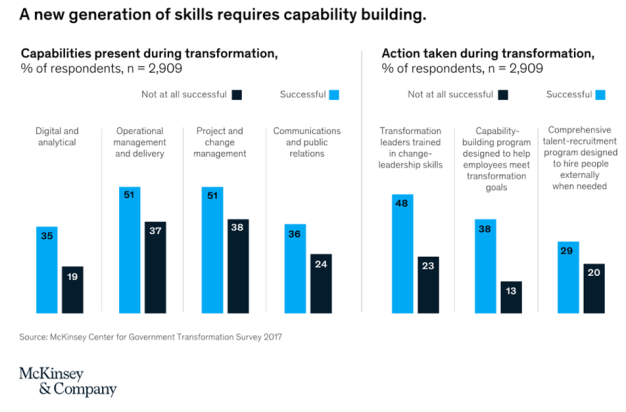
None of this is easy: indeed, leading a large-scale change effort is a huge personal challenge for any senior government official. Few governments train their leaders sufficiently in the people skills needed: research by the McKinsey Center for Government (MCG) finds that fewer than a third of public-sector transformation leaders have received any training in change-leadership skills. And findings from a McKinsey survey of public- and private-sector organizations suggest that public-sector managers typically fall short in at least three important interpersonal-skill dimensions: giving feedback, motivating employees, and supporting their development. Public-sector participants in the survey were less likely than the average participant to agree that managers at their organizations were trained in these skills (Exhibit 3).
Exhibit 3
To build the leadership skills and mind-sets needed to inspire and sustain change, we recommend three key interventions whose impact has been proven across many transformation efforts.
The first is bringing senior transformation leaders together. Leading a transformation can be an isolating, unfamiliar experience; with some notable exceptions, few public servants lead more than one agency or department in their career. Many of the senior leaders we interviewed emphasized that they lacked a network of peers with whom to test ideas and share experiences. That meant they were forced to learn on the job when the stakes were extremely high. To address this challenge, some governments have created special forums to bring together leaders from across ministries and agencies to develop critical skills—and build networks to support change efforts for years to come. For example, the government of New Zealand introduced its senior civil-service leaders to digital and innovation concepts via a full-day executive class that covered topics such as digitization best practices and hiring digital talent. The training also included a live “hackathon” that allowed the participants to redesign and digitize a series of citizen interactions, using agile methods.
That points to a second key step: designing leadership-training programs that go beyond theory and give participants opportunities to practice and hone new skills in real-world settings. We have seen several public organizations follow a “field-and-forum” approach to capability building. Instead of simply providing training and assuming it will trickle into organizational practices, a field-and-forum approach provides classroom training in a series of workshops and then takes a structured approach to translating the theory into practice via hands-on projects in the field. A European labor agency, for instance, used this approach to train more than 150 managers. After the program was completed, 93 percent of participants reported that they were inspired to implement new capabilities in their daily work.
The third key thrust for leaders of transformation is to develop the skills and nurture the passion, to communicate in an inspirational way with all the groups affected by the change—especially the organization’s own employees. Of course, every government communicates, but only a few cut through the noise effectively enough to win hearts and minds. Many government institutions continue to be hierarchical organizations that follow the protocol of top-down, one-way communication cascades on the assumption that civil servants simply need clear instructions in order to act effectively. However, two-way communication and genuine engagement are what they need. The findings of MCG’s Government Transformation Survey underline this truth: in the most successful transformations, the senior-management team communicated openly and across the organization about its progress. And nearly 90 percent of transformation participants said success would have been enhanced by engaging more regularly with frontline employees.
Unlike governments’ private-sector counterparts, those that fail to deliver do not “go out of business”—and their employees are unlikely to lose their jobs. That, combined with the societal impact that effective government transformation achieves, has important implications for how public-sector leaders create internal motivation for employees to change: they must be adept at framing the transformation in a positive way. Rachna Gandhi of Service NSW put it this way: “We weren’t going out to our front line and saying that we really want to drive digital adoption, and them feeling the threat of, ‘does this mean we will have no jobs?’ We went and said customers want more digital; we’ve got to train them on this. How will we go about it?”
Just as governments need to invest in their leaders’ transformation skills, they must build capabilities for change across the organization—from the team tasked with managing the transformation program right through to the front line. MCG’s research shows that capability-building programs designed to help employees meet transformation goals more than triple the success rate of public-sector change initiatives.
So what kinds of capability programs are required? Certainly not the training in the policy and diplomacy skills classically emphasized in government. Rather, capability building is needed in a new generation of skills in operational delivery, analytics, change management, and communications (Exhibit 4). These new skills require new investment—which might mean that governments need to reverse the trend of declining public spending on labor-force training and support that has been observed in most Organisation for Economic Co-operation and Development (OECD) countries over the past 20 years.1 Governments will also need to reallocate training budgets from compliance-based training to programs that nurture the skills that are critical to support transformation. In Ireland, for example, government leaders have explicitly committed more time and resources to training: they have increased the government’s learning-and-development budget to more than 3 percent of payroll, with a focus on critical skills such as digital capabilities.
Exhibit 4
But public-sector leaders need to do much more than shift training budgets: they need to shift cultures. One leader we interviewed spoke for many of his public-sector peers when he said, “I’ve spent my life not developing these skills. In fact, I have been advised against taking roles [that] focus on these, as they are less highly valued.”
Moreover, as we noted previously, public-sector organizations typically need to prioritize capability building more than their private-sector counterparts, as employee development and coaching in government has generally been less robust. For example, a McKinsey survey found that just 28 percent of public-sector managers were trained in supporting employees’ development, compared with 41 percent of managers across all sectors. Likewise, as Exhibit 3 shows, public-sector managers were much less likely to be trained in giving employees feedback.
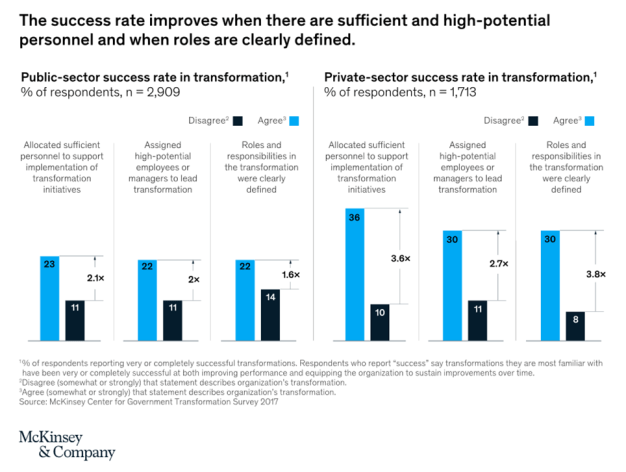
Beyond these broader steps in capability building, governments must also home in on the teams tasked with managing the transformation effort. It’s critical to ensure that these teams are staffed with high-potential employees with clearly defined roles and responsibilities—and that the employees are trained effectively to deliver on those responsibilities (Exhibit 5). When governments get that right, they can double the success rate of large-scale change efforts.
Exhibit 5
All around the world, governments and public-sector agencies face an urgent imperative to deliver better outcomes, improve citizens’ experience of public services, and make constrained budgets go further. Achieving these results calls for ambitious, large-scale transformation. To get major change programs right, however, governments need to focus relentlessly on the three Ps: people, people, and people. They need to understand and tackle the cultural factors that hold back change, build change-leadership skills and mind-sets among senior managers, and nurture new capabilities right across their organizations.
Article link: https://www.mckinsey.com/industries/public-sector/our-insights/putting-people-at-the-heart-of-public-sector-transformations
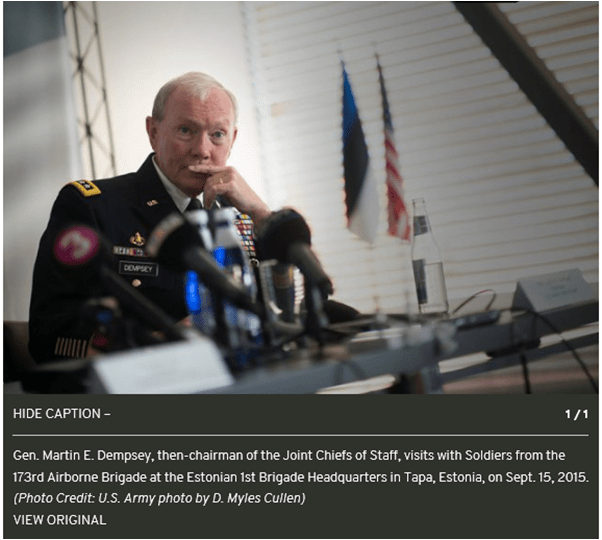
WASHINGTON — When it comes to building teams, few people have more experience than Retired Gen. Martin E. Dempsey. Across his 41-year career, which culminated with being the 18th chairman of the Joint Chiefs of Staff, Gen. Dempsey was known as a Soldier’s Soldier and was revered by those he led. A graduate of the U.S. Military Academy, he also served as the 37th chief of staff of the Army and as commander of both Training and Doctrine Command and U.S. Central Command. We sat down with him to discuss his take on building the Army team for the future.
Q: You held many key leadership positions throughout your career. What were some of the lessons you learned about building successful teams?
A: For leaders at every level, from the lowest tactical level all the way up through the Army’s senior leadership, I think the best approach is to first think about how you influence before exerting your authority. To me, the best kind of leadership establishes a sense of belonging, makes clear that everyone’s contribution matters, and creates an environment where people get the job done because the leader has been persuasive with them.
The way you create high performing organizations that are cohesive and collaborative is by thinking about leadership as influence rather than authority. As soon as you have to exert authority, your leadership has become directive and the team responds differently.
There are obviously times when you have to exert your authority because there’s inadequate time to be influential and persuasive. But in the normal course of events, if you are a leader who believes in getting things done through influence, you’ll build the kind of trust that will allow the unit to respond positively when you do have to exert authority.
Q: How would you describe your leadership philosophy?
A: In the kind of leadership environment we live in, one with ubiquitous information, fragile facts, and intense scrutiny, the way to achieve trust within an organization is by being inclusive. I just coauthored a book, titled “Radical Inclusion,” because I believe this so strongly.
As we transitioned to an all-volunteer force, we made a commitment to ensure it would be reflective of the society it serves. That took us down a path of making sure we had a diverse group of leaders in the formations based on gender, ethnicity, and so forth. I think we really made impressive progress.
But let me make a distinction here. The kind of thing we’re talking about is beyond simple diversity. It’s not just taking stock of whether you have the proper representation of ethnic groups or genders, but, rather, we should be focusing on how inclusive we are. If you’re inclusive, the organization will naturally feel like it is contributing and bringing meaning, not just being dragged around by leadership.
Q: Can you discuss the importance of responsibility as it relates to maximizing team performance and realizing potential?
A: Responsibility is one of the principles of our profession; leaders accept responsibility for outcomes. This means they don’t just simply pass the buck. At every level, leaders need to hold themselves accountable for what they can, and should, accomplish at their particular level, whether it’s something as mundane as maintenance rates or something as abstract as building the Iraqi army. When they don’t have what they need to do so, they have an obligation to make sure the chain of command is informed.
The military can sometimes be criticized for its “can do” attitude. You’ve probably never met an officer who would say, “No, I can’t do that.” But we actually have a responsibility to explain both what we can do and what we can’t. That responsibility is at every level of the organization.
Of all the jobs I had in my career, the one with the least authority was actually when I was chairman of the Joint Chiefs of Staff. All the budgetary authority flows through the service chiefs; all the operational authority flows through the combatant commanders and up through the secretary of defense and the president. So the chairman’s role in some ways is to balance the supply and demand aspects of the force to meet the demands of the combatant commanders to the greatest extent possible, while making sure the service chiefs have the ability to develop forces ready to carry out the combatant commanders’ intent.
But that’s where responsibility comes in. It would be irresponsible to allow that relationship to become out of balance. If we constantly consume the force as it becomes ready, it makes it almost impossible for the service chiefs to organize, train, and equip the force as well as educate it on the responsibilities of the profession, its role in society, and its relationship with the American people. It is the chairman’s primary responsibility to keep all of that in balance.
Q: How important is sustainment to our operations, and how did you ensure our logisticians were integrated into the joint and coalition teams?
A: Absolutely vital. A famous logistician back in the Desert Storm era made the apropos comment that logisticians draw a line in the sand beyond which the operators dare not tread. His point was, generally speaking, logistics will determine the capability, speed, and tempo of operations. While that quote was very famous back in the 1990s, I had a much different view. I felt it was a bit pejorative and negative, suggestive that the logisticians were a limiting factor of what we could do. Throughout my entire career, I instead preferred to look at sustainment and logistics as enabling factors.
To ensure they’re integrated into the team, you have to include them at every point in the planning, preparation, and execution of the mission. As a battalion and regimental commander, I never allowed my staff to concoct an operations plan, get my approval on it, and then toss it over the transom to the logisticians and say, “Figure out how you’re going to support this.” Sustainers had to be on the team from the start so we had diverse thinking about these complex challenges.
I personally think that’s even more important today. The problems we face are so much more complex, especially in deployments, both the kind we’ve already fought and the ones we prepare for but have not had to perform yet, such as establishing a base of operation in Europe. That was one of the things I worried about most as chairman.
We had become exclusively capable at the kind of missions we were running in Iraq and Afghanistan but had let some of our expertise in other areas erode, things like the value and importance of deterrence, the ability to set a theater, and the ability to maneuver over distance with a heavy force and ensure all the enablers could move at the same pace. I think the expertise is starting to be regenerated, but we can never take those things for granted. Those who sustain and those who are storming the hill better be involved in the planning and preparation from the beginning, or in execution it’ll fail.
Q: Can you discuss the role our military spouses and Families play in the success of our total Army?
A: In 2003, I was commander of the 1st Armored Division and was given responsibility for Baghdad. Our mission statement for Task Force Iron was to establish a safe and secure environment in which the duly-appointed government of Iraq could restore basic services and security. We were spread out all over the place with more than 50 combat outposts and forward operating bases, and I had 32,000 Soldiers.
As I told my junior leaders, one of the things we learned very quickly was that contrary to other wars, we really took our Families with us when we deployed. They all looked at me like I had lost my mind, but my point was that we now had Soldiers either texting, Skyping or FaceTiming with their Families all the time. It was, “Oh by the way, I have to go now because I’ve got to take a convoy out; I’ll text or come back up on Skype when I get back.” So family members now had a real-time sense of anxiety about the well-being of their Soldiers.
It was interesting back in those days to try to exert some control over that. Finally, I came to the conclusion — and this gets back to the idea of radical inclusion — that the answer wasn’t to try to control it because it became nearly impossible. Even if you thought you could, you couldn’t. Instead, we actually tried to empower it and to literally make the family members feel like part of the team by sharing information with them about what we were doing and why. It became a very powerful leadership tool.
Initially, we thought the division was going home by Christmas of 2003. That was extended to April, which brought us to one full year, and then we were extended again to July following the Shiite rise. The way we got through that was making sure Soldiers and their Families concurrently understood what was happening and why.
I sent Mark Hertling, a brigadier general at the time, back to Europe, where we were mostly based, to partner with my wife, the U.S. Army Europe commander, and the European installation management director. Together they went from kaserne to kaserne doing hour-and-a-half briefings and taking another hour’s worth of questions so Families understood why our mission was important. Those Families then became part of the solution, not part of the problem.
As a commander at any level, if you think you can just worry about those who wear the uniform, it’s a big mistake.
Q: What was the most challenging team-building experience you had?
A: The most challenging experiences are generally those where units come together on relatively short notice, as we experienced in particular during the first decade of this century with things like the surge in Iraq. Everyone in the Army at the time was trying to figure out how we could more quickly adapt and innovate and how we could become more agile. One of the answers that emerged was modularity.
As we began to go down that path, phrases like “plug and play” came into play. We would take brigade combat teams from various divisions, run them through a mission readiness exercise, and then deploy them. But the cost of this model in terms of team building was pretty high.
Throughout the first 20 or 30 years of my career, I belonged to units that trained together habitually. We were task-organized habitually; we always knew which tank company would go over to the Infantry brigade or which Infantry battalion would come over to the Armor brigade, and we trained that way year-round. We got to know each other; our Families got to know each other. When you have that kind of constant interaction, it builds a bond of trust that runs pretty deep.
Modularity, of course, is kind of the antithesis of that. People come and go based on the needs of a particular mission. It’s the ultimate exercise in task organization. That’s difficult because systems or units only become high-performing when they begin to trust each other, not before. As an Army, I think we have to constantly be conscious of this balance between agility that comes through modularity and the bonding that comes through continuity.
Q: Since retiring from service, has your outlook on leadership evolved?
A: If anything, my beliefs about leadership based on my experiences coming through the ranks have actually been reinforced, especially this idea of trust being the cornerstone of building teams. In today’s environment, political corrosiveness has caused having a pleasant conversation about issues, which was always challenging, to become seemingly impossible. We often talk less about the substantive issues than we do about the narrative that accompanies them. It’s a battle of competing narratives more than a battle of merit on a particular issue. In that environment, it makes leading more difficult. Fortunately, however, it doesn’t make it impossible.
What makes it possible is a commitment to creating a sense of belonging, to make sure people know their contributions matter, and to develop trust. That was how I tried to lead throughout my career, particularly as a general officer where all of the sudden I had influence on the future of the Army and joint force. I’m sure there were individual actions along the way that I would’ve liked to have come out differently, but in terms of how I tried to build teams, I don’t think I would’ve done anything differently.
Q: What is the most important thing a young Soldier should know as part of the larger Army team?
A: The best young leaders, be they enlisted, warrant officers, or commissioned officers, have always had a sense that they were part of something bigger than themselves. I personally believe one of the things that makes the Army special is this ability to recognize the greater good we serve, and that’s probably even more true today in the current environment.
It doesn’t come to life immediately when a young man or woman raises their hand and takes the oath. But if leaders feel that responsibility to continue to educate the force that this is a team of teams, I think we’re going to be okay. We can’t forget we are one joint force, and it’s the American people who are counting on us. If we stay true to our professional ethos, we will succeed.
——————–
Arpi Dilanian is a strategic analyst in the Army G-4’s Logistics Initiatives Group. She holds a bachelor’s degree from American University and a master’s degree from Rensselaer Polytechnic Institute.
Matthew Howard is a strategic analyst in the Army G-4’s Logistics Initiatives Group. He holds bachelor’s and master’s degrees from Georgetown University.
——————–
This article was published in the November-December 2018 issue of Army Sustainment.
Article link: https://www.army.mil/article/213079/radical_inclusion_an_interview_with_retired_gen_martin_dempsey
