After a five-year fight, the Virginia legislature voted this week to expand the Medicaid program to an estimated 400,000 low-income residents who are not currently eligible for health coverage. And New Jersey became the second state to impose a state-level “individual mandate” requiring most residents to have health insurance or pay a fine, following last year’s repeal of the federal penalty.
Meanwhile, Congress has quietly passed a major bipartisan bill to overhaul and streamline health programs provided to the nation’s veterans. The bill includes an expansion of veterans’ ability to get private care paid for outside the Department of Veterans Affairs system, in certain cases.
Also this week, an interview with Dr. Arthur Kellerman, dean of the Uniformed Services University of the Health Sciences, the military’s medical school in Bethesda, Md.
This week’s panelists for KHN’s “What the Health?” are Julie Rovner of Kaiser Health News, Joanne Kenen of Politico, Paige Winfield Cunningham of The Washington Post and Rebecca Adams of CQ Roll Call.
Among the takeaways from this week’s podcast:
Two key factors helped push Medicaid expansion through the Virginia General Assembly. One was the Trump administration’s endorsement of work requirements for nondisabled adults and the other was the blue wave that shook the state last November when the House of Delegates nearly turned from a safe Republican majority to Democratic control.
New Jersey’s passage of a mandate that state residents get coverage or face a penalty was surprising because that provision was one of the most disliked parts of the federal Affordable Care Act.
Even as Congress sent the president the bill expanding VA programs, there is a widening debate in Washington about whether the system should be privatized. That debate has helped both create the vacancy at the top of the Department of Veterans Affairs and complicated efforts to fill it.
Plus, for “extra credit,” the panelists recommend their favorite health stories of the week they think you should read, too.
Julie Rovner: Bloomberg News’ “Is There a Doctor Aboard? Airlines Often Hope Not,” by Ivan Levingston
Joanne Kenen: The Atlantic’s “Ambien Doesn’t Cause Racism,” by Olga Khazan
Rebecca Adams: ProPublica’s “Why Your Health Insurer Doesn’t Care About Your Big Bills,” by Marshall Allen
Paige Winfield Cunningham: The New York Times’ “Origins of an Epidemic: Purdue Pharma Knew Its Opioids Were Widely Abused,” by Barry Meier
Also: The New Yorker’s “The Family That Built an Empire of Pain,” by Patrick Radden Keefe
Dr. Nikhil Wagle thought he had a brilliant idea to advance research and patient care.
Dr. Wagle, an oncologist at the Dana Farber Cancer Institute in Boston, and his colleagues would build a huge database that linked cancer patients’ medical records, treatments and outcomes with their genetic backgrounds and the genetics of their tumors.
The database would also include patients’ own experiences. How ill did they feel with the treatments? What was their quality of life? The database would find patterns that would tell doctors what treatment was best for each patient and what patients might expect.
The holdup, he thought, would be finding patients. Instead, the real impediment turned out to be gathering their medical records.
In the United States, there is no single format used by all providers, and hospitals have no incentive to make it easy to transfer records from one place to another. The medical records mess is hobbling research and impeding attempts to improve patient care.
“Data are trapped,” said Dr. Ned Sharpless, director of the National Cancer Institute. “This is a huge problem. It is phenomenally important.”
The cancer institute has invested millions of dollars into determining the genetic sequences of patients’ tumors, and researchers have found thousands of genes that seem to drive tumor growth.
But until patients’ medical records are linked to the genetic data, life-or-death questions cannot be answered.
“What drug did they get? Did they respond? Did they survive? Were they cured?” Dr. Sharpless asked.
The federal government has mandated uniform standards for electronic health records. “At this point, they are not to a level that helps with the detailed clinical data that we need for the scientific questions we want to ask,” Dr. Wagle said.
A few private companies are trying to tackle the problem. Flatiron Health, just bought by Roche, has obtained about 2.2 million records of cancer patients from medical centers and made them available for research after stripping them of identifiable information.
But Flatiron must employ 900 nurses and certified tumor registrars, people with master’s degrees in coding data, to put it all into a usable form.
“About 50 percent, if not more, of the critical details we need for research are trapped in unstructured documents,” said Dr. Amy Abernethy, the company’s chief medical officer.
“They are in PDFs. Maybe a doctor put in a note by hand, maybe a doctor typed it. That note became a narrative. It is not something that can easily be put into a spreadsheet.”
Dr. Sharpless worries that the data acquired by companies like Flatiron will not be readily available to researchers. But if the companies manage to solve the medical records problem cheaply, he said, “we’d like to work with them to figure out how to liberate the data.”
Dr. Wagle is making data from medical records and patients’ experiences public as he gets them. After 2 1/2 years, though, he is disappointed by how little there is to share.
The patient who inspired his project had a lethal form of thyroid cancer. She was expected to die in a few months. In desperation, doctors gave her a drug that by all accounts should not have helped.
To everyone’s surprise, her tumors shrank to almost nothing, and she survived. She was an “extraordinary responder.”
Why? It turned out that her tumor had an unusual mutation that made it vulnerable to the drug.
And that got Dr. Wagle thinking. What if researchers had a database that would allow them to find these lucky patients, examine their tumors, and discover genetic mutations that predict which drugs will work?
And what about those who were not helped by standard treatments? Could they be identified and spared treatments that will not work?
What researchers needed was a huge database that collected clinical and genetic data, along with patients’ descriptions of their experiences. Those narratives are crucial, Dr. Wagle said, but they are absent from the commercial databases like Flatiron’s. Those comprise anonymous patient data, making it impossible to ask the patients themselves how they fared.
Dr. Wagle decided to build a database, starting with metastatic breast cancer, his specialty. There are about 155,000 metastatic breast cancer patients in the United States. He would use social media, online forums and advocacy groups to reach out to patients for their records.
The Metastatic Breast Cancer Project began in October 2015. Patients have been eager to join, and advocacy groups enthusiastically signed on. So far, the project includes 4,400 women.
Determining the genetic sequences of their tumors and of their healthy cells was straightforward — “the easy part,” Dr. Wagle said.
Gathering their medical records was another story. The data exist in all sorts of formats, and crucial information may be missing altogether.
Simply getting the records delivered, in whatever format, has been a nightmare. Records usually arrive as faxes or via snail mail.
“Even though the patients are saying, ‘I have consented for you to obtain my medical records,’ there is no good way to get them,” Dr. Wagle said.
He hired half a dozen people to work full-time on the project, and corralled doctors and other experts to help part-time. It can take hours to go through a single medical record.
Mary McGillicuddy, who works full-time on the project, explained the system. When patients enroll, they tell the investigators where they were treated, where they had biopsies, where they had scans, and where they had medical procedures.
They give Ms. McGillicuddy and her colleagues permission to request their records. Ms. McGillicuddy faxes requests for records to each medical institution that treated a patient, or diagnosed or sequenced her cancer.
Startlingly, faxing “is the standard,” Ms. McGillicuddy said, for medical records requests.
The process can be frustrating. Fax numbers can be out of date. Some medical centers will not accept electronic patient signatures on the permission forms.
Sometimes, the medical centers just ignore the request — and the second request. In the end, Ms. McGillicuddy said, the project gets fewer than half the records it requests.
Then comes the laborious task of extracting medical information from the records and entering it into the database. A faxed medical record may be 100 or 200 pages long.
So far, the breast cancer project has received 450 records for 375 patients. (Each patient tends to have more than one record, because the women typically are seen at more than one medical center.)
“Patients are incredibly engaged and excited,” Dr. Wagle said. But for the records problem, “right now there isn’t a good solution.”
Correction:
An earlier version of this article described incorrectly Dr. Amy Abernethy’s role at Flatiron Health. She is its chief medical officer, not its founder. In addition, the article misstated the number of medical records obtained by the company. The figure is 2.2 million, not 1 million.
VA Video Connect can be used by any veteran who has video-capable technology — such as a smartphone, tablet or computer.
For many veterans, communicating with a doctor in real time will now be as convenient as putting a new app on their smartphone, tablet or personal computer.
VA Video Connect, which the U.S. Department of Veterans Affairs (VA) began piloting in 2017, is now being rolled out to veterans across the country. The service enables veterans to interact with their physicians using a secure video connection to address nearly any issue that does not require an in-person visit.
The app can be used by any veteran who has video-capable technology — such as a smartphone, tablet or computer — a reliable internet connection, and access to a VA provider who uses the service. The VA began rolling out Video Connect in July 2017; as of April 20, 4,500 VA providers had used it to communicate with more than 22,500 veterans. The VA hopes that increased use of Video Connect will help relieve some of the agency’s wait time and access issues.
The new service has already demonstrated its capabilities. When VA Video Connect was being piloted last year, its introduction coincided with the devastation left behind by hurricanes Harvey and Irma. Video Connect enabled VA physicians to remotely get veterans the care they needed, underscoring its potential to reach patients unable to physically travel because of their disability or distance from their doctor.
The service is also valuable to veterans who have mental health issues. It can put patients in virtual touch with psychiatrists and counselors, bypassing the often long waits for appointments. “Having that availability is important, whether in person or through telemedicine,” says Garry Augustine, executive director of DAV (Disabled American Veterans), a nonprofit organization that provides services for and lobbies on behalf of more than a million wounded veterans. “It’s a good option for times when a vet needs to be able to talk to a professional quickly,” Augustine says.
Telemedicine is not a new service for the VA. According to a spokesperson, the department pioneered telemedicine nearly 60 years ago, using closed-circuit television to connect a mental health therapist with a group of veterans gathered in a remote location. By 2006, advancements in technology allowed the VA to enable physicians to use telemedicine to screen veterans in remote medical facilities for conditions such as diabetic eye disease.
Today, the VA offers telemedicine services in more than 50 clinical specialty areas, such as wound care and dermatology. VA physicians conduct millions of remote visits each year. In fiscal year 2017, more than 727,000 veterans used VA tele-health services in medical facilities, representing more than 2.18 million episodes of care. Now that access is spreading to veterans’ personal devices.
VA Video Connect works on any device that has an internet connection, a web camera, a microphone and speakers. It is available in the Apple App Store for iPhones and iPads. On personal computers and Android or Windows mobile devices, VA Video Connect operates as a web-based app, and it does not require an app download. To determine whether a device is compatible with VA Video Connect, veterans can visit the VA Video Connect test site.
In a past era, the work of the hospital physician was done primarily at the bedside or in the adjacent wet laboratory. Residents had the opportunity to witness the unfolding of diseases (for which we may now have cures) and to come to know their patients over the course of lengthy hospitalizations. The life was grueling and all-consuming — and those who took it up were almost invariably unmarried white men, with teaching hospitals actively discouraging marriage. Medicine was a fraternal order. Doctors’ lounges were central locations where community internists, specialists, and surgeons ate together, socialized, and “curbsided” each other for patient consultations. Charts were kept on paper and were often indecipherable.
Every aspect of medicine and training has since evolved. Progress has been remarkably quick in some areas and painfully slow in others. The past 20 years have seen much debate over the amount of time worked by house staff. As residents’ duty hours have changed, so has the nature of their work.
Typically in our field, internal medicine, residents arrive at the hospital at 7 a.m., get sign-outs from nighttime residents, and conduct “pre-rounds” to see patients they have inherited but don’t know well, before heading to morning report or attending rounds. Attending rounds often consist of “card-flipping” sessions held in a workroom, frequently interrupted by discharge planning and pages, calls, and texts from nurses and specialists. Finalizing discharges before noon can feel more important than getting to know new patients. Increasingly, the attending physician doesn’t see patients with the team, given the time constraints.
No longer are there paper charts at the bedside. The advent of the electronic era, while reducing the time required for tracking down laboratory or radiology results, has not substantially changed the time spent with patients: recent estimates indicate that medical students and residents often spend more than 40 to 50% of their day in front of a computer screen filling out documentation, reviewing charts, and placing orders. They spend much of the rest of their time on the phone coordinating care with specialists, pharmacists, nutritionists, primary care offices, family members, social workers, nurses, and care coordinators; very few meetings with these people occur face-to-face. Somewhat surprisingly, the time spent with patients has remained stable over the past six decades.1
The skills learned early by today’s medical students and house staff — because they are critical to getting the work done — are not those needed to perform a good physical exam or take a history, but rather the arts of efficient “chart biopsy,” order entry, documentation, and sign-out in the electronic age. When a medical team gets notice of a new admission, it seems instinctive and necessary to study the patient’s record before meeting him or her. This “flipped patient” approach2 has advantages, but it introduces a framing bias and dilutes independent assessment and confirmation of history or physical findings.
In short, the majority of what we define as “work” takes place away from the patient, in workrooms and on computers. Our attention is so frequently diverted from the lives, bodies, and souls of the people entrusted to our care that the doctor focused on the screen rather than the patient has become a cultural cliché. As technology has allowed us to care for patients at a distance from the bedside and the nursing staff, we’ve distanced ourselves from the personhood, the embodied identity, of patients, as well as from our colleagues, to do our work on the computer.
But what is the actual work of a physician? Medical students entering the wards for the first time recognize a dysjunction, seeing that physicians’ work has less to do with patients than they had imagined. The skills they learned in courses on physical diagnosis or communication are unlikely to improve. Despite all the rhetoric about “patient-centered care,” the patient is not at the center of things.
Meanwhile, drop-down menus, cut-and-paste text fields, and lists populated with a keystroke have created a medical record that (at least in documenting the physical exam) at best reads like fiction or meaningless repetition of facts and at worst amounts to misleading inaccuracies or fraud. Given the quantity of information and discrepancies within medical records, it’s often impossible to discern any signal in the mountains of noise. Yet our entire health care system — including its financing, accounting, research, and quality reporting — rests heavily on this digital representation of the patient, the iPatient, and provides incentives for its creation and maintenance.3 It would appear from our hospital quality reports that iPatients uniformly get wonderful care; the experiences of actual patients are a different question.
It’s clear that physicians are increasingly dissatisfied with their work, resentful of the time required to transcribe and translate information for the computer and the fact that, in that sense, the work never stops. Burnout is widespread in the workforce, and more than a quarter of residents have depression or depressive symptoms.4 In response, health care leaders have advocated amending the “Triple Aim” of enhancing patients’ experience, improving population health, and reducing costs to add a fourth goal: improving the work life of the people who deliver care.
A 2013 study commissioned by the American Medical Association highlights some of the factors associated with higher professional satisfaction. Perhaps not surprisingly, the investigators found that perceptions of higher quality of care, autonomy, leadership, collegiality, fairness, and respect were critical. The report highlighted persistent problems with the usability of electronic health records as a “unique and vexing challenge.”5
These findings underscore the importance of reflecting on what our work once was, what it now is, and what it should be. Regardless of whatever nobility inhered in the work of physicians in a bygone era, that work was done under conditions and quality standards that would now be unacceptable. We practice in a safer and more efficient system with measurable outcomes. Yet with the current rates of burnout, our expectations for finding meaning in our profession and careers seem largely unfulfilled.
We believe that if meaning is to be restored, the changes needed are complex and will have to be made nationally, beginning with a dialogue that includes the people on medicine’s front lines. Perhaps the greatest opportunity for improving our professional satisfaction in the short term lies in restoring our connections with one another. We could work on rebuilding our practices and physical spaces to promote the sorts of human connections that can sustain us — between physicians and patients, physicians and physicians, and physicians and nurses. We could get back to the bedside with patients, families, and nurses. We could get to know our colleagues from other specialties in shared lunchrooms or meeting spaces.
In addition, we believe that in the coming years, the U.S. medical community will have to rethink the human–computer interface and more thoughtfully merge the real patient with the iPatient. We have an opportunity to radically redesign electronic health record systems, initially created for fee-for-service billing, as our organizations shift toward bundled payments, capitation, and risk sharing. Perhaps virtual scribes and artificial intelligence will eventually reduce our documentation burden.
But technology cannot restore our professional satisfaction. Our profession will have to rebuild a sense of teamwork, community, and the ties that bind us together as human beings. We believe that will require spending more time with each other and with our patients, restoring some rituals that are meaningful to both us and the people we care for and eliminating those that are not.
Solutions will not be easy, since the problems are entangled in the high cost of health care, reimbursement for our work, and obstacles to health care reform. But we can start by recalling the original purpose of physicians’ work: to witness others’ suffering and provide comfort and care. That remains the privilege at the heart of the medical profession.
Disclosure forms provided by the authors are available at NEJM.org.
November 10, 2016
N Engl J Med 2016; 375:1813-1815
DOI: 10.1056/NEJMp1609055
From the Section of General Internal Medicine, Yale University School of Medicine, New Haven, CT (D.I.R.); and the Program in Bedside Medicine, Department of Medicine, Stanford University School of Medicine, Stanford, CA (A.V.).
Czernik Z, Lin CT. A piece of my mind: time at the bedside (computing). JAMA2016;315:2399–2400
Chi J, Verghese A. Clinical education and the electronic health record: the flipped patient. JAMA2014;312:2331–2332
Verghese A. Culture shock — patient as icon, icon as patient. N Engl J Med2008;359:2748–2751
Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA2015;314:2373–2383
Friedberg MW, Chen PG, Van Busum KR, et al. Factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Santa Monica, CA: RAND, 2013 (http://www.rand.org/pubs/research_reports/RR439.html).
Third-party payment programs make health insurance affordable for low-income consumers by paying the health plan premium costs not covered by the ACA’s tax credits
Third-party payment programs not only help low-income Americans afford marketplace health coverage, they also reduce hospitals’ uncompensated care costs
Abstract
Issue: Consumers’ concerns about affordability limit participation in ACA marketplaces. Funded by local hospital systems and run by independent nonprofits, third-party payment (TPP) programs improve affordability for low-income consumers by paying premium costs not covered by tax credits.
Goal: To assess the potential of TPP to make marketplace coverage more affordable, without harming insurance risk pools.
Methods: Interviews in May and June 2016 with program administrators, hospital systems, carriers, and consumer groups in five localities and the Washington State marketplace.
Key Findings: The most effective local program reached 1,148 people, or 25 percent of all eligible marketplace enrollees. Other local programs served between 202 and 934 consumers; the Washington State program reached 1,133. Findings suggest that without TPP, numerous beneficiaries would have remained uninsured. Hospitals funding these programs reported net financial benefits, with declines in uncompensated care exceeding program costs. Carriers reported no adverse selection in these carefully designed programs. Conclusions: Widespread adoption of TPP could help additional low-income consumers obtain marketplace coverage. Hospitals’ financial gains from TPP programs make replication more feasible. However, broader policies, such as increased premium tax credits and cost-sharing reductions, are likely needed for major nationwide improvements to affordability.
Introduction
With roughly 20 million Americans gaining coverage under the Affordable Care Act (ACA), the United States has made enormous progress in reducing the number of uninsured.1 Nevertheless, 28.6 million people remained without health coverage in 2016,2 of whom an estimated 62 percent qualified for Medicaid or marketplace coverage.3 As of June 2015, only 35 percent of consumers eligible for advance premium tax credits — which lower monthly health insurance payments — had enrolled in marketplace plans.4 Research suggests that the most important obstacle to increased enrollment has been consumers’ belief that coverage is unaffordable.5
Currently, the future of the ACA remains unresolved, but the basic framework of the legislation could well remain intact. If so, stakeholders and policymakers will need to revisit these affordability concerns. A fully effective solution would likely include higher premium tax credits and cost-sharing reductions. Until such a solution is considered, more incremental strategies may be needed, like third-party payment (TPP) programs, through which health care providers pay low-income consumers’ share of enrollment costs.
History suggests that TPP programs can address low-income consumers’ affordability concerns on a large scale. Long before the ACA, Washington State’s Basic Health Program let nonprofit organizations pay the premium charges of eligible consumers using donations from safety-net providers. The state stopped most new enrollment in the early 2000s. Before then, this TPP initiative achieved significant gains, enrolling nearly a quarter of all 133,000 consumers who received subsidized coverage when the state’s Basic Health Program reached its high-water mark in 2001.6
Some carriers have expressed concerns that TPP programs could skew risk pools by triggering “adverse selection,” or disproportionately high enrollment of consumers with serious health problems. For example, carriers have raised concerns about health care providers increasing their payments for kidney dialysis and other high-cost conditions by steering patients who qualify for Medicaid or Medicare to nonprofit organizations, which in turn enroll the patients into marketplace plans that pay higher reimbursement rates.7 After seeing “problematic” effects on consumers and risk pools, the Centers for Medicare and Medicaid Services (CMS) circulated regulations in late 2016 limiting TPP programs that focus on dialysis patients.8 Those regulations soon became the subject of litigation,9 and a broader policy debate continues around TPP programs that serve patients with specific diagnoses.10
This issue brief focuses on different TPP programs: those that base eligibility on income rather than the presence of particular health conditions. Based on interviews conducted in May and June 2016 with nonprofit program administrators, hospital systems, carriers, and consumer groups in five localities and the Washington State marketplace, we examine whether income-based TPP programs can improve enrollment and retention without triggering harmful adverse selection.11 We also explore whether income-based TPP programs could be implemented on a much larger scale. For detailed information on our methods, see How We Conducted This Study.
Catherine H. MacLean, M.D., Ph.D., Eve A. Kerr, M.D., M.P.H., and Amir Qaseem, M.D., Ph.D., M.H.A.
Performance measurement in the U.S. health care system has expanded dramatically over the past 30 years. The National Quality Measures Clearinghouse now lists more than 2500 performance measures. These measures are used in various quality-reporting, accountability, and payment programs sponsored by commercial payers, government agencies, and independent quality-assessment organizations. The Centers for Medicare and Medicaid Services (CMS) aims to base 90% of Medicare fee-for-service payments to clinicians on “value” by the end of 2018 by using performance scores.
Although most physicians view the delivery of high-quality care as a professional imperative,1 performance-measurement activities face increasing resistance from physicians and some policymakers who believe that current measures are not meaningful.2 In a recent survey, 63% of physicians said that current measures do not capture the quality of the care that physicians provide.3 Yet U.S. physician practices are spending $15.4 billion each year — about $40,000 per physician — to report on performance.3
In response to these concerns, the Performance Measurement Committee (PMC) of the American College of Physicians (ACP) developed criteria to assess the validity of performance measures (see box). Using a modified version of the method developed at RAND and UCLA for evaluating the benefits and harms of a medical intervention, we applied the ACP criteria to the measures included in the Medicare Merit-based Incentive Payment System (MIPS)/Quality Payment Program (QPP). We hypothesized that if most of the MIPS/QPP measures assessed were deemed valid using this process, physicians could have more confidence that adherence to the measured practices would result in improved patient outcomes. Conversely, if some substantial proportion of the measures were deemed not valid, the results would suggest the need to change the process by which MIPS measures are developed and selected. (For further details, see the methods section in the Supplementary Appendix, available at NEJM.org.)
ACP Measure Review Criteria.
Domain 1. Importance
Meaningful clinical impact: Implementation of the measure will lead to a measurable and meaningful improvement in clinical outcomes.
High impact: Measure addresses a clinical condition that is high-impact (e.g., high prevalence, high morbidity or mortality, high severity of illness, and major patient or societal consequences).
Performance gap: Current performance does not meet best practices, and there is opportunity for improvement.
Domain 2. Appropriate Care
Overuse: Measure will promote stopping use of a test or treatment in general population or individuals where the potential harms outweigh the potential benefits.
Underuse: Measure will encourage use of a test or treatment in general population or individuals in whom the potential benefits outweigh the potential harms.
Time interval: Time interval to measure the intervention is evidence-based.
Domain 3. Clinical Evidence Base
Source: Evidence forming the basis of the measure is clearly defined with appropriate references.
Evidence: Evidence is high-quality, high-quantity, and consistent and represents current clinical knowledge.
Domain 4. Measure Specifications
Clarity — numerator and denominator clearly defined:
For process measures, numerator includes a specific action that will benefit the patient, and denominator includes well-specified exclusions.
• For outcome measures, numerators detail an outcome that is meaningful to the patient and under the influence of medical care.
• Denominator includes well-specified and clinically appropriate exceptions to eligibility for the measure.
Clarity — all components necessary to implement measure clearly defined
Validity: The measure is correctly assessing what it is designed to measure, adequately distinguishing good and poor quality.
Reliability: Measurement is repeatable and precise, including when data are extracted by different people.
Risk adjustment: Risk adjustment is adequately specified for outcome measures.
Domain 5. Measure Feasibility and Applicability
Attribution: Level of attribution specified in the measure is appropriate (measure ties the outcomes to the appropriate unit of analysis) and is clearly stated.
Physician’s control: Performance measure addresses an intervention that is under the influence of the physician being assessed.
Usability: Results of the measure provide information that will help the physician to improve care.
Burden: Data collection is feasible and burden is acceptable (low, moderate, or high)
Of 271 measures in the 2017 QPP measures list, we identified and rated the validity of 86 that the committee considered relevant to ambulatory general internal medicine. Among these, 32 (37%) were rated as valid by our method, 30 (35%) as not valid, and 24 (28%) as of uncertain validity. We also determined the proportion of the measures that had been developed by the National Committee for Quality Assurance (NCQA) or endorsed by the National Quality Forum (NQF) that were rated as valid by our method. As compared with measures that were not endorsed by these organizations, greater percentages of NCQA-developed and NQF-endorsed measures were deemed valid (59% and 48%, respectively, vs. 27% for nonendorsed measures), and smaller percentages were deemed not valid (7% and 22%, vs. 49% for nonendorsed measures). (For further details on the measure review results, see the tables in the Supplementary Appendix.)
Ratings for a Sample of Measures.
For each measure, the committee rated validity with respect to five domains: importance, appropriateness, clinical evidence, specifications, and feasibility and applicability. Examples of the overall and domain ratings given to individual measures judged to be valid, not valid, and of uncertain validity are shown in the table.
Notably, among the 30 measures rated as not valid, 19 were judged to have insufficient evidence to support them. For example, MIPS measure 181, “Elder Maltreatment Screen and Follow-Up,” requires the completion of the Maltreatment Screening tool on the date of an encounter and a documented follow-up plan for all patients 65 years of age or older. Although elder abuse is a serious problem that physicians should appropriately diagnose and report, the U.S. Preventive Services Task Force has found insufficient evidence to warrant routine screening. We believe the substantial resources required to screen large populations of elderly patients for maltreatment and to track follow-up would be better directed at care processes whose link to improved health is supported by more robust evidence.
Another characteristic of measures that were not rated as valid by our method was inadequately specified exclusions, resulting in a requirement that a process or outcome occur across broad groups of patients, including patients who might not benefit. MIPS measure 236, “Controlling High Blood Pressure,” for instance, requires that a blood pressure of 140/90 mm Hg or lower be achieved in the clinic setting for all patients. Forcing blood pressure down to this threshold could harm frail elderly adults and patients with certain coexisting conditions.
We also identified measures that were directed at important, evidence-based quality concepts but had poor specifications that might misclassify high-quality care as low-quality care. For example, MIPS measure 009, “Anti-depressant Medication Management,” assesses whether patients who started taking an antidepressant medication continued taking one at 3 and 6 months after initiation. This measure does not consider patients’ reasonable preferences for switching to alternative, evidence-based interventions such as psychotherapy or electroconvulsive therapy after experiencing side effects of antidepressants.
Our analysis identified troubling inconsistencies among leading U.S. organizations in judgments of the validity of measures of physician quality. Although the ACP assessment was limited to a defined set of measures, that set was large and included the vast majority of measures that will be applied to ambulatory care internists as part of the United States’ largest physician quality-assessment program for the purpose of accountability. Our findings are striking given that the criteria we used were similar to those used by NQF and CMS. Why the disconnect?
Possible explanations include the methods used to assess measures and the characteristics of the experts who did the assessing. The RAND–UCLA appropriateness method does not classify measures as valid when there are significant disagreements among the panelists. In contrast, the NQF threshold for endorsement is close to a simple majority of panelists (60%). The ACP method thus sets a higher standard for validity. In addition, we would argue that the RAND–UCLA method can be considered more evidence-based than other methods, since favorable clinical outcomes have been demonstrated for patients treated according to standards developed with this method.4,5
It is also possible that the perspectives of the groups doing the rating contribute to differences in validity ratings. Specifically, NQF convenes multistakeholder groups, whereas the ACP committee is composed exclusively of physicians with expertise in clinical medicine and research. However, analyses of the RAND–UCLA method in which multiple panels were convened to rate identical criteria have demonstrated high levels of agreement across panels for necessary care. Hence, although changing the panel composition might result in some differences in ratings, we would not expect the variation to be large enough to explain why so many NQF-endorsed measures were rated as not valid by the ACP committee.
The fact that only 37% of measures proposed for a national value-based purchasing program were found to be valid with a standardized method has implications for physician-level performance measurement. The use of flawed measures is not only frustrating to physicians but also potentially harmful to patients. Moreover, such activities introduce inefficiencies and administrative costs into a health system widely regarded as too expensive. If developers, assessors, and public and private payers adopted a more rigorous method of assessing measures’ validity, potential problems could be identified before the measures were launched. It makes sense for practicing clinicians to participate in the development and review of measures. At the same time, a single set of standards (like those put forth by the National Academy of Medicine for clinical practice guidelines) could be developed that would allow others to evaluate the trustworthiness of performance measures.
We believe that the next generation of performance measurement should not be limited by the use of easy-to-obtain (e.g., administrative) data or function as a stand-alone, retrospective exercise. Instead, it should be fully integrated into care delivery, where it would effectively and efficiently address the most pressing performance gaps and direct quality improvement. For now, we need a time-out during which to assess and revise our approach to physician performance measurement.
Disclosure forms provided by the authors are available at NEJM.org.
This article was published on April 18, 2018, at NEJM.org.
Author Affiliations
From the Center for the Advancement of Value in Musculoskeletal Care, Hospital for Special Surgery, New York (C.H.M.); the University of Michigan Department of Internal Medicine and Institute for Healthcare Policy and Innovation and the Veterans Affairs Ann Arbor Center for Clinical Management and Research, Ann Arbor (E.A.K.); and the American College of Physicians, Philadelphia (A.Q.); and the ACP Performance Measurement Committee (C.H.M., E.A.K.). The other members of the Performance Measurement Committee were J. Thomas Cross, Jr., Eileen Barrett, Robert Centor, Andrew Dunn, Nick Fitterman, Bruce Leff, Ana María López, Mark Metersky, Robert Pendleton, Stephen D. Persell, Edmondo J. Robinson, Sameer D. Saini, Paul Shekelle, and from the American College of Physicians, Sarah Dinwiddie.
Qaseem A, Snow V, Gosfield A, et al. Pay for performance through the lens of medical professionalism. Ann Intern Med 2010;152:366–369.
2. Berwick DM. Era 3 for medicine and health care. JAMA 2016;315:1329–1330.
3. Casalino LP, Gans D, Weber R, et al. US physician practices spend more than $15.4 billion annually to report quality measures. Health Aff (Millwood) 2016;35:401–406.
4. Higashi T, Shekelle PG, Adams JL, et al. Quality of care is associated with survival in vulnerable older patients. Ann Intern Med 2005;143:274–281.
5. Hemingway H, Crook AM, Feder G, et al. Underuse of coronary revascularization procedures in patients considered appropriate candidates for revascularization. N Engl J Med 2001;344:645–654.
Transforming Care focuses on new models of care, payment approaches, and patient engagement strategies that have the potential to reshape our delivery system to better meet the needs of the nation’s sickest and most vulnerable patients.
March 29, 2018 Issue
In Focus: Increasing Collaboration Among Physicians, Hospitals, and Postacute Providers to Reduce Variation and Spending
While many U.S. hospitals have concentrated on improving care transitions from hospital to home, far fewer have focused on the transition from hospitals to postacute care settings, including skilled nursing facilities. Increased awareness of variations in spending on postacute care and avoidable complications after hospital discharge — together with value-based payment arrangements — have prompted some physician groups, health systems, health plans, and postacute care providers to collaborate. Among their methods: assessing patients’ risk and identifying the most appropriate setting for them to recover and offering education to help patients regain their functionality and stay well. Better data about what works best for different patients and more aligned financial incentives among acute and postacute care providers could further these efforts.
By Martha Hostetter and Sarah Klein
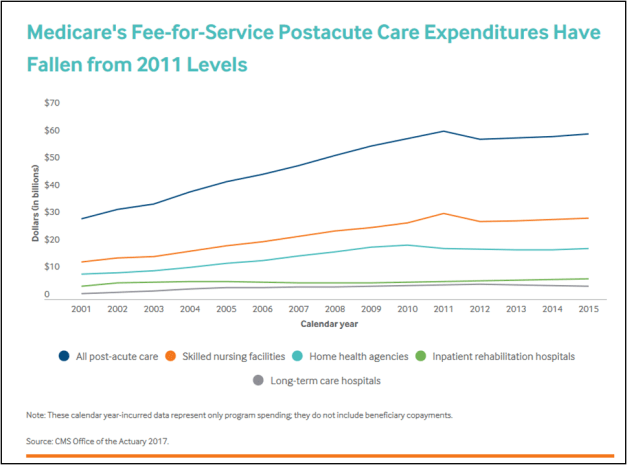
The Institute of Medicine’s 2013 study of Medicare spending upended a common assumption about the biggest drivers of regional variation: it was not hospital use that accounted for the largest the differences in spending across regions, but what happened after patients emerged from hospitals and began making use of skilled nursing facilities (SNFs) and home health care. The report also traced the dramatic rise in spending on SNF use and other types of postacute care, which more than doubled from 2001 to 2011, making it the fastest-growing sector of health care.1
The rise in the use of postacute care can be traced to Medicare’s decision in the 1980s to stop paying hospitals on a fee-for-service basis and instead make payments based on patients’ diagnoses, not how long they stay. This, together with the increased prevalence of capitated payments under managed care in the 1990s, led hospitals to reduce lengths of stay. Both factors fueled demand for postacute care providers — which include skilled nursing facilities (SNFs), home health agencies, inpatient and outpatient rehab facilities, and long-term hospitals — to help patients recover after surgery or acute illness and return home.2 Demand for postacute care also increased as a function of the aging of the U.S. population and the increasing prevalence of chronic and disabling conditions, which complicate recovery.3 About two of five Medicare beneficiaries end up needing some form of postacute care after a hospitalization.4