It was supposed to be a miracle, but now it’s what keeps Laura Bush, a nurse-practitioner near Albuquerque, awake at night.
There’s a drug called Sovaldi that works astonishingly well to cure people with the liver disease Hepatitis C. The rub? It costs $1,000 per day for all 12 weeks of treatment.
Bush’s clinic, First Choice Community Healthcare, is a federally qualified health center in the rural town of Los Lunas, New Mexico, which means she sees a disproportionate number of patients who are uninsured, underinsured, and on Medicaid, the government insurance program for the poor. In other words, they can’t afford Sovaldi.
The state’s Medicaid program rations access to Sovaldi and other blockbuster Hep C drugs to only the sickest patients. Even with those limitations, the drugs will likely cost the state an estimated $140 million this year. At various points since Sovaldi became available last year, Bush said, Medicaid has required her to perform risky liver biopsies on patients to prove how sick they are, or wait until patients have late-stage liver disease before they can be eligible for coverage. Each day, Bush juggles seeing patients with writing appeal letters and filing pre-authorizations that are often denied.
“Imagine if you went to get your mammogram, and they said, ‘you’ve got this [lump] here, but we’re not going to do anything about it until it gets bigger,’” Bush told me recently. “How would you take that, as a patient?”
With enough paperwork and tenacity, for a while Bush was able to secure free doses of Sovaldi directly from its manufacturer, Gilead Sciences. But that strategy, too, has become tougher in recent months after Gilead limited the types of patients who could receive free drugs.
New Mexico health-care workers aren’t the only ones struggling to secure these new treatments for their patients. Other states also require patients to be in late-stage liver disease, get urine drug screens, or prove abstinence from drugs and alcohol before they’ll consider covering them. Hep C patients commonly find themselves being forced to get sicker before they can get better.
Hep C is a liver disease transmitted by blood. It’s most common among baby boomers, most of whom contracted it through blood transfusions or by using contaminated needles to inject drugs. Left untreated, Hep C attacks the liver and can lead to cancer or liver failure.
Sovaldi costs $84,000 for a 12-week course of treatment, or about $1,000 per pill. It’s a great drug, working nearly 90 percent of the time and with few side effects. Sovaldi and the similarly pricey Harvoni, also made by Gilead, are a big improvement over older cures like interferon, which was only effective about half the time and whose side effects—rashes, fever, and nausea—were sometimes described as worse than the disease itself.
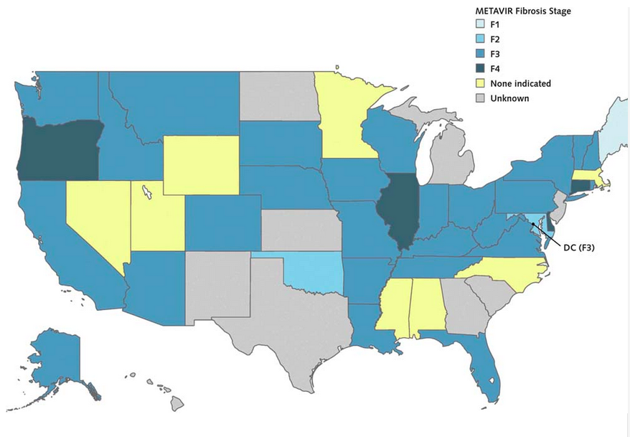
If state governments were to pay for Sovaldi or Harvoni for all of the Hep C patients on their Medicaid and prison rolls, the total bill would have been $55 billion. Most state Medicaid programs, therefore, are sharply limiting access to them. An August study in the Annals of Internal Medicine found that most states were only making these new drugs available to Medicaid patients who had advanced fibrosis, or liver scarring. Two-thirds required urine drug tests for drugs and alcohol before they would cover the medication. These measures, the study notes, are inconsistent with the recommendations of prominent health organizations and FDA guidelines.
Liver Disease Required for Medicaid Coverage of Sovaldi
State Medicaid programs, meanwhile, feel their hands are tied. “The states can’t afford it,” said Matt Salo, executive director of the National Association of State Medicaid Directors. “If we were to pony up for [Sovaldi], we would spend as much on this one drug as we would for all other drugs in the entire program. We don’t have the luxury of having a state legislature saying, ‘You want 5 to 10 percent more [money] this year? Cool, here’s your money.’ Many state legislatures are saying, ‘You’ve got to save, because revenues are down.’”
* * *
Martin Shkreli, the 32-year-old head of Turing Pharmaceuticals, stoked Internet outrage this week when it was reported that he raised the price of the 62-year-old anti-parasite drug Daraprim to $750 per tablet, from $13.50. Then he defended himself, Gekko-style, by saying, “I am a capitalist who plays to win.”
On Wednesday, he said he’ll lower the price to an undisclosed amount, but not before the parasite-free-organs-are-for-closers attitude drew widespread attention to the rising cost of prescription drugs. The prices of existing medications for everything from tuberculosis to blood pressure have rocketed up in recent years after the drugs were acquired by pharmaceutical companies.
“[Daraprim] is such a perfect, crystalline example of everything that can be done, given the lack of rationality in the system, and the total bankruptcy of the justifications for high drug prices in the first place,” Peter B. Bach, director of the center for health policy and outcomes at Memorial Sloan Kettering Cancer Center in New York, told the Washington Post.
But price hikes on existing drugs represent just a small part of America’s overall prescription-cost woes. Drug companies are regularly churning out new medications to treat everything from cholesterol to cancer. The $84,000 Sovaldi is practically nothing, for example, compared to Solirism, a $700,000-per-year drug that treats a rare blood disease, or Naglazyme, a $500,000 treatment for a rare skeletal disorder. The difference is that unlike drugs that only a few hundred Americans will ever need, Sovaldi could completely change the lives of the roughly three million Hep C sufferers in the U.S.
If, that is, their insurers would pay for it.
“I will at all costs try to get you the medication.”
Drug makers have long justified their high prices by saying it’s the only way they can recoup their investment into research and development. Then again, pharmaceutical companies have some of the largest profit margins in the health-care industry.
In an emailed statement, a Gilead spokeswoman responded to questions about Sovaldi’s price by saying, “unlike treatment for other chronic diseases, Sovaldi offers a cure … at a price that significantly reduces Hepatitis C treatment costs and delivers significant savings to the healthcare system over the long-term.”
Together, Sovaldi and Harvoni generated $12.4 billion in sales for Gilead last year. The company’s CEO, John C. Martin, is a billionaire. Gilead’s revenues doubled last year, and as the New York Times wrote, the company “now is faced with figuring out what to do with all the cash it is generating.”
* * *
Last year, New Mexico’s Human Services Department issued a rule that required patients to show that they have Stage 3 or Stage 4 liver fibrosis before Medicaid will cover them for drugs like Sovaldi.
In Stage 4, the liver is “hard as a rock,” Sanjeev Arora, a University of New Mexico physician, told the Albuquerque Journal. “Treating someone for Hepatitis C after they have developed cirrhosis is a little bit like closing the barn door after the horse has left.” While they wait to develop cirrhosis, Hep C patients face a higher risk of developing depression, nerve pain, and lymphoma.
When low-income Hep C patients come to see Bush, she’ll assure them that she wants to see them cured. “I will at all costs try to get you the medication,” she says.
If the person doesn’t have cirrhosis, she asks them to write a letter describing why they need Sovaldi. She’ll fill out a prior authorization and send it to Medicaid. If Medicaid denies the request, as she says often happens, she appeals. And on it goes.
Those who don’t get the medication can die “some of the worse deaths I’ve ever seen,” Bush said. People with end-stage liver disease vomit blood, feel confused, and turn yellow and bloated. “At the end you die not knowing who you are, your belly looks 12 months pregnant, you’re malnourished, and you’re bleeding to death,” she said.
Bush currently has about 20 patients waiting to get Sovaldi. One man doesn’t yet have cirrhosis, but he has trouble swallowing. His insurance won’t cover Sovaldi, which is a single-pill regimen, but will pay for a different treatment that requires taking multiple pills. Bush is worried he’ll choke.
Previously, Gilead sometimes provided free Sovaldi treatments to poor people who had been denied access to the drug by their insurer. But in July, the company changed its criteria and now only extends that offer to people who are uninsured. In the statement to The Atlantic, the Gilead spokeswoman said that the change was a response to insurers who were refusing to pay for Sovaldi. The assistance program “was designed to help uninsured patients with the most need, and changes are necessary to remain true to that mission,” she said.
Sovaldi’s story is not unique in America, but it is a uniquely American story. Other countries rigorously regulate the prices of prescription drugs, just as American cities set the rates of public utilities. In Germany, for example, the insurance-like “sickness funds” negotiate with both physician groups and drug manufacturers to determine the costs of all treatments. In the U.S., meanwhile, drug makers can simply name their price.
Sometimes, all of her attempts fail, and Bush has to tell her patients she can’t get one of these miracle pills for them. “I have one patient who got so upset because she thought I was blocking her ability to get the meds,” Bush said. “She came to me and said, ‘no one wants to give me the medications because I’m poor.’”
That woman finally did receive the drug, Bush said. It took seven months.
Article link: http://www.theatlantic.com/health/archive/2015/09/an-expensive-medications-human-cost/407299/