


The more I study digital transformation, the more I realize that it’s not mostly about either “digital” or “transformation.”
1) Digital transformation is not about technology. A key misconception about digital transformation is that it is something that companies choose to do with technology or is primarily about their implementation and use of technology.
It isn’t.
Instead, digital transformation is about how technology changes the conditions under which business is done, in ways that change the expectations of customers, partners, and employees.
For example, the rise of new disruptive businesses like Uber Technologies Inc. and Lyft Inc. resulted in large part from changes in the technological infrastructure that were not initiated by the company’s founders. Instead, these startups recognized that the widespread adoption of personal mobile devices equipped with certain features provided new opportunities to bring people together to exchange goods and services. They responded to these opportunities by developing novel services that catered to changing customer (and driver) expectations. The success of these platforms further changed business conditions, creating even more new opportunities. For instance, the New York-based restaurant technology company Mobo Systems Inc., doing business as Olo, is building upon the Uber platform to offer restaurant delivery that relies on Uber drivers as delivery people.
So, while Uber, Lyft, and Olo are certainly technology companies, at least in part, the more significant technological shifts that gave rise to their businesses were those over which they had little influence and took place before the companies were founded. Likewise, many of the most significant technological changes to the competitive environment your company faces lay outside your control, but they are created by a pervasive digital infrastructure that continues to evolve. The key question of digital transformation is whether you are paying close enough attention to these changes to respond to the resulting changes in expectations of customers, partners, and employees for how business is done — or whether a competitor or a startup will respond first?
2) Digital transformation is not about transformation. Looking up a number of definitions for the word “transformation” demonstrates that they exhibit a common characteristic — they all define transformation as a singular process that occurs and is then completed.
Digital transformation, however, does not work that way. It is not a process that will ever be complete, at least not in the near future. Moore’s Law continues to suggest that processing power per dollar doubles every 18 months. Storage capacity and networking speeds increase at an even faster rate (doubling every 12 and nine months, respectively). New classes of technologies — artificial intelligence, blockchain, autonomous vehicles, augmented and virtual reality — will likely become widely adopted over the coming decade or two, fundamentally changing expectations yet again. By the time you adapt to today’s digital environment, that environment will have likely already changed significantly.
What is digital transformation about, then?
At its most fundamental level, digital transformation is about the ability of organizations, its leaders and employees, to adapt to rapid changes wrought by evolving digital technologies. Thus, understanding digital transformation is both good news and bad news.
It’s good news in the sense that all companies can make the types of changes necessary to become more digitally mature. Digitally mature organizations exhibit certain organizational similarities that have nothing to do with technology. For example, our 2017 report on digital business notes that digitally mature companies tend to be organized into cross-functional teams Last year’s report found that digitally mature companies had a distinct set of cultural characteristics, and throughout our research we have found that employees of all ages want to work for digitally mature companies. All companies can develop these traits.
It’s bad news in the sense that almost all companies find these types of changes to their culture, talent, and structure to be difficult to accomplish. Organizations typically change much more slowly than technology does, and these types of changes will not happen without the intentional effort to make them happen. Furthermore, organizations tend to become more static over time, so the necessary adaptability can be difficult to maintain even if it is established.
What can companies, leaders, and employees do now?
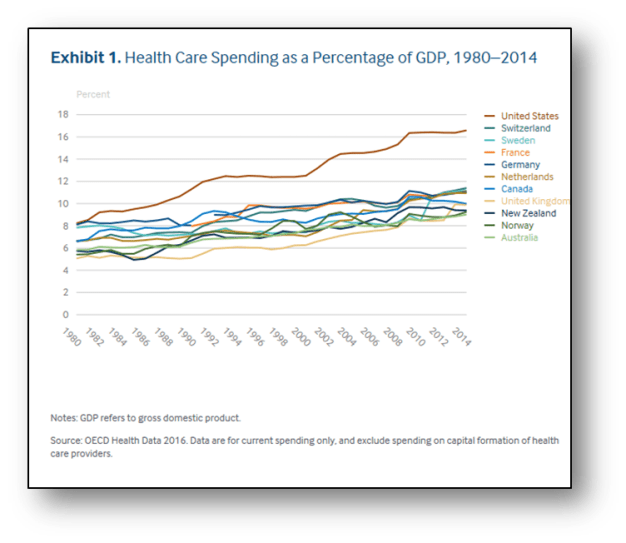
The United States spends far more on health care than other high-income countries, with spending levels that rose continuously over the past three decades (Exhibit 1). Yet the U.S. population has poorer health than other countries. 1 Life expectancy, after improving for several decades, worsened in recent years for some populations, aggravated by the opioid crisis. 2 In addition, as the baby boom population ages, more people in the U.S.—and all over the world—are living with age-related disabilities and chronic disease, placing pressure on health care systems to respond.
Timely and accessible health care could mitigate many of these challenges, but the U.S. health care system falls short, failing to deliver indicated services reliably to all who could benefit. 3 In particular, poor access to primary care has contributed to inadequate prevention and management of chronic diseases, delayed diagnoses, incomplete adherence to treatments, wasteful overuse of drugs and technologies, and coordination and safety problems.
This report uses recent data to compare health care system performance in the U.S. with that of 10 other high-income countries and considers the different approaches to health care organization and delivery that can contribute to top performance. We based our analysis on 72 indicators that measure performance in five domains important to policymakers, providers, patients, and the public: Care Process, Access, Administrative Efficiency, Equity, and Health Care Outcomes.
Our data come from a variety of sources. One is comparative survey research. Since 1998, The Commonwealth Fund, in collaboration with international partners, has supported surveys of patients and primary care physicians in advanced countries, collecting information for a standardized set of metrics on health system performance. Other comparative data are drawn from the most recent reports of the Organization for Economic Cooperation and Development (OECD), the European Observatory on Health Systems and Policies, and the World Health Organization (WHO).
Read Full Article: http://www.commonwealthfund.org/interactives/2017/july/mirror-mirror/

Forbes is out with its annual list of richest people in tech, and it updates the estimated net worth of Epic Systems founder and CEO Judy Faulkner to $3.4 billion.
Forbes’ previous estimate had been $2.4 billion.
Not bad for someone who started her EHR software company in a basement. That was in 1979. Today, Faulkner has sold electronic health record systems to some of the most prestigious healthcare systems in the country, and Epic reportedly has 53 percent of the market.
Epic is a privately held company and the software maker says she wouldn’t have it any other way.
At HIMSS17 last February, Faulkner announced she had two new EHR options in development.
Faulkner is giving away her billions. She signed the Giving Pledge in 2015, promising to donate 99 percent of her fortune to philanthropic causes within her lifetime. Faulkner is No 73 on the Richest in Tech List.
Other healthcare tech billionaires include Microsoft founder Bill Gates, who is maintaining his No.1 spot with $84.5 billion. He and his wife, Melinda Gates, have also signed the Giving Pledge to give away their fortune. Gates gave $4.6 billion to charity earlier this month. It was his biggest donation since 2000.
Dell Technologies CEO Michael Dell is No. 10 on the Forbes list with $22.6 billion. He started his business 33 years ago – in his dorm room.
 Building on an increasingly sophisticated understanding of naturally occurring biological processes, researchers have developed technologies to predictably modify or create organisms or biological components. This research, known collectively as synthetic biology, is being pursued for a variety of purposes, from reducing the burden of disease to improving agricultural yields to remediating pollution. While synthetic biology is being pursued primarily for beneficial and legitimate purposes, it is possible to imagine malicious uses that could threaten human health or military readiness and performance. Making informed decisions about how to address such concerns requires a comprehensive, realistic assessment. To this end, the U.S. Department of Defense, working with other agencies involved in biodefense, asked the National Academies of Sciences, Engineering, and Medicine to develop a framework to guide an assessment of the security concerns related to advances in synthetic biology, to assess the level of concern warranted for various advances and identify areas of vulnerability, and to
Building on an increasingly sophisticated understanding of naturally occurring biological processes, researchers have developed technologies to predictably modify or create organisms or biological components. This research, known collectively as synthetic biology, is being pursued for a variety of purposes, from reducing the burden of disease to improving agricultural yields to remediating pollution. While synthetic biology is being pursued primarily for beneficial and legitimate purposes, it is possible to imagine malicious uses that could threaten human health or military readiness and performance. Making informed decisions about how to address such concerns requires a comprehensive, realistic assessment. To this end, the U.S. Department of Defense, working with other agencies involved in biodefense, asked the National Academies of Sciences, Engineering, and Medicine to develop a framework to guide an assessment of the security concerns related to advances in synthetic biology, to assess the level of concern warranted for various advances and identify areas of vulnerability, and to
prioritize options to address these vulnerabilities.
This interim report proposes a framework

Several dozen federal technologists, chief information officers and acquisition experts have developed a guidebook for how agencies ought to pursue cloud-based solutions.
Nextgov obtained a draft copy of the guide, which was authored in partnership with an interagency group comprised of tech leaders from the Defense Department, Federal Communications Commission, General Services Administration and other agencies.
The stated purpose of the CASTLE (short for Cloud Acquisition Professionals Cloud Adoption Survival Tips, Lessons, and Experiences) guide is to “allow agencies to mitigate and smooth the acquisition process, thus increasing adoption of cloud services within the federal government.”
» Get the best federal technology news and ideas delivered right to your inbox. Sign up here.
At more than 20,000 words, the guidebook contains granular analysis and nuanced discussion regarding various approaches, frameworks and implementations agencies have used toward procuring cloud services. Users can navigate the document based on various conditions, such as funding models, and view acquisition information and possible frameworks associated with each.
Members have been sharing the draft with federal technology and industry leaders in an effort to solicit further feedback, improve upon the draft and attract attention and buy-in from the White House in hopes of driving new policy measures.
“I’m not saying I’m going to stand outside Jared Kushner’s house until he gets a copy, but the narrative we’ve created in this guide needs the audience and support of the Office of Management and Budget and groups like the White House Office of American Innovation,” said Sarah Millican, a digital strategy adviser for the FCC’s Office of the CIO and outreach leader for the interagency Cloud Computing Center of Excellence. “This guide was created because we thought the ‘modernizing legacy IT in government’ ball should’ve been further down the field.”
Millican told Nextgov the guide book’s goal—to help government modernize its systems more quickly—mirrors broader initiatives put forth by the Jared Kushner-led White House Office of American Innovation. Kushner, President Donald Trump’s son-in-law, has described the new office as a “SWAT team” for government efficiency and has used the White House’s convening power to gather feedback from tech industry CEOs.
This input, however, comes from civil servants who’ve been tackling cloud computing projects since cloud became a thing and whose battle to modernize government from the trenches goes back more than a decade, according to David Bray.
“This is the trench-level implementer’s perspective, and we’re sharing it upward,” said Bray, who has served as executive chairman of the interagency group since its inception. With Bray’s recent exit to the private sector, Chad Sheridan, CIO at the Agriculture Department’s Risk Management Agency, is expected to take on the role in late September.
Succinctly, Sheridan described the document as a “research-driven guide addressing the hurdles the federal government faces when trying to modernize legacy IT.” He said it establishes a common vocabulary for sometimes nebulous concepts like cloud, acquisition and security, and allows feds testing the cloud services waters to review pros, cons, challenges and possible solutions to various approaches they might take. It also provides perspectives relevant for various personnel in the technology procurement chain, including program managers, executives and acquisition staff.
“The agency may then leverage the information provided within the guide as acquisition-based guidance, but will need to tailor and supplement the information. The guide takes a narrow scope which includes targeted acquisition based topics that have proven to be problematic in the procurement of cloud computing services,” the draft document states. “Agency stakeholders are able to match key attributes of their agency’s expected situation to attributes of the provided scenarios that illuminates potential guidelines, considerations, and a path forward for their agency.”
Trump’s budget proposal calls for an increase in cloud spending, allocating $8.5 billion of a total $95.7 billion federal IT budget for provisioned services such as cloud computing. Yet that’s a paltry amount compared to the 75 percent of the IT budget that the Government Accountability Office estimates agencies will spend on aging, legacy IT systems. Many mission-critical IT systems across government are more than 40 years old.
Yet even as the federal cloud computing market has grown, agencies have been far less aggressive in adopting cloud services than private-sector counterparts. The CASTLE guide addresses several barriers to the government realizing cloud computing’s potential to reduce IT spend and reduce reliance on old data centers.
This guide addresses the ambiguity over cloud computing’s definition, disconnect over how providers market cloud services to government customers, and explains security and consumption-based pricing models previously foreign to government.
Yet the draft document indicates most challenges “are not technical in nature, but the result of cultural constraints.”
In the coming weeks, the interagency group plans to begin soliciting feedback from cloud service vendors and industry representatives. On Sept. 27, the group plans to host a working-group meeting, inviting government members and industry reps to discuss next steps.
Representation from the White House would be welcome, Millican said.
She, along with Bray and others, have suggested the government ought to aim to move 75 percent or more of its civilian IT systems to the cloud by 2019.
“For [the White House] to join up with GSA and tackle this moon-shot of a goal for government to be 75 percent cloud in two or three years would be a game-changer,” Millican said.
Open source software helps organizations improve their health IT infrastructure technology faster at a lower cost.

August 16, 2017 – Health IT infrastructure is advancing quickly and organizations must keep up with the most up-to-date technology innovations while still trying to save money.
Open source software is gaining popularity in the healthcare space because it naturally lends itself to innovation, Red Hat Director of Healthcare Craig Klein told HITInfrastructure.com.
“Open source is a methodology on how to develop software,” Klein explained. “The premise behind open source is you have a group of people collaborating on a particular piece of code. For example, if you have someone building an operating system, there may be one hundred thousand people contributing that particular piece of code from thousands of organizations.”
The open source community takes the code that’s being worked on and releases it into open source projects.
Klein emphasized that there are several different kinds of open source, which has caused healthcare organizations to be skeptical when first considering the technology for their IT infrastructure.
READ MORE: Open Source Blockchain Development Critical to Standardization
There’s open source that is in the open source community that are projects. Then there’s open source that is enterprise-grade.
Healthcare companies should not develop on community-based open source because there aren’t usually companies behind it to secure and support it. Making the open source code enterprise grade is what allows healthcare organizations to use it in a commercial environment.
Enterprise grade open source can be used successfully in healthcare because the open source code is taken by a vendor and made secure for enterprise. Enterprise grade open source is what allows open source software to be HIPAA compliant.
“Five or six years ago, organizations were very concerned about security with open source, but the opposite is actually true,” Klein stated. “There are so many people looking at the code that open source code is more secure than a proprietary code.”
“I don’t hear security concerns much anymore and organizations are really looking at open source as a way to secure things better than just having a proprietary environment because there are more people working on it.”
READ MORE: Top Considerations for Choosing a Cloud EHR Infrastructure
Open source is the key to fast health IT innovation that will help healthcare defeat some of its biggest technological challenges, such as interoperability and security.
“Open Source is used a lot of different ways in healthcare,” said Klein. “The best way to understand why it’s been doing so well in the healthcare world is to think about how doctors work. “
“Doctors collaborate and get together with other doctors of similar specialties and different specialties,” he continued. “Their theory is if you have more people working on the problem you’re going to find a better solution. There’s specialist working with general practitioners and multiple specialist working on a single case.”
“The same is true with open source,” Klein added. “There’s multiple people working on a similar problem. It’s a natural fit into healthcare clinicians understand the open source development model.”
Open source also helps organizations save money in the face of value-based care by allowing them to continue using legacy pieces of their health IT infrastructures while also incorporating new technology advancements.
READ MORE: Benefits of Open-Source Software to Healthcare Community
“Open source allows you to work with other vendors so when the software is developed, it’s developed to work with everything,” Klein explained. “When organizations deploy open source, it makes it much easier to share data and information and to integrate. Interoperability is all about open source, which is absolutely critical in healthcare.”
Open source also plays a significant role in healthcare analytics, mobility, cloud, and virtualization.
“If you look at all the big data players in healthcare, they’re all open source based companies,” said Klein. “Most of the technology being developed, whether it be big data, analytics, mobile, or software-defined networks, all this development is happening in the open source world, which perfectly fits with all the interoperability needs within healthcare.”
“Most of the major cloud environments, around 80 percent, are developed and run on open source environments,” he continued. “There’s a tremendous need in healthcare for flexibility and the ability to adapt to all changes and take advantage of the cloud. The cloud world is driven by open source as is the need to be flexible enough to work with older and newer technologies and open source allows you to do that.”
Open source also has a large part to play in the development of future technologies that will continue to help healthcare organizations use technological advancements to benefit both clinicians and patients.
“A lot of the innovations taking place in IT are happening in the open source world,” Klein explained. “It just makes sense. My theory is that one company just isn’t large enough to come up with all the things that need to happen. That’s why open source is becoming such a big factor in the marketplace. We’ll continue to see open source becomes more and more prevalent. People are asking for it because of the speed of innovation and the flexibility.”
“Healthcare organizations cannot afford to get rid of all their old technology so they’re in a sort of hybrid mode,” he continued. “Open source allows them to take advantage of using all the technology together which is why it’s growing more popular in healthcare.”
Open source has a lot to offer healthcare but it cannot be successful without careful consideration of an entity’s future.
“Putting an open source piece here and there is nice, but it’s not going to take you where you want to go,” Klein advised. “Organizations need to look at where their future state wants to be what open source can do for them. This determines the best places to use the technology in conjunction with what’s already there.”
“It’s basically looking at an overall plan and determining where the openness and flexibility is needed, and apply it there as an overall strategy. Entities can’t just throw everything out and start over again.”
Healthcare organizations stand to gain a lot from open source technology in terms of innovation and technological advancements. This option also caters to value-based care and getting the most out of an IT infrastructure budget.
“Open source allows organizations to work with other vendors so when open source software is developed, it’s developed to work with everything,” Klein concluded. “When entities deploy open source, it makes it much easier to share data and information and to integrate health IT systems.”
Article link: https://hitinfrastructure.com/news/why-open-source-software-fits-health-it-infrastructure

Now that Republicans in Congress appear to have at least temporarily abandoned their crusade against the Affordable Care Act, it seems like a good time for lawmakers to come up with plans to fulfill their promises to increase access to health care and to lower costs.
Let’s stipulate up front that congressional leaders and President Trump are unlikely to lead that effort, given that they narrowly failed to take health insurance away from millions of people. This conversation would need to be led by senators who have committed to a bipartisan approach, and by state governments, some of which have already begun to take action.
Change might not come soon enough for the 29 million people without health insurance or the many millions who struggle to afford high premiums, deductibles and other health costs. But even the A.C.A., the 2010 health law also known as Obamacare, was the product of many years of spadework and was based on a Massachusetts health reform bill signed into law by Gov. Mitt Romney in 2006.
Obamacare has helped 20 million people gain access to insurance, and it appears to have helped slow the growth in health care costs. But even former President Barack Obama has said that there is still work to be done. The United States spends much more on medical care than other rich countries, like Britain, Australia and the Netherlands, according to a recent Commonwealth Fund report, yet its citizens live shorter lives and suffer from more illnesses and injuries than people in other industrialized nations.
One option that appears to have gained support among the public is a single-payer system, which proponents like Senators Bernie Sanders and Elizabeth Warren call “Medicare for All.” A Kaiser Family Foundation poll found in June that 53 percent of Americans favor such a system. This was up from 46 percent, according to an average of seven polls conducted in 2008 and 2009. But moving to a single-payer system from one dominated by employer-paid health coverage would be a big leap, and in any case the political climate is clearly not ready for it. Many Democratic voters as well as party leaders like Representative Nancy Pelosi and Senator Chuck Schumer have been reluctant to embrace the idea, and, no surprise, most Republican voters and lawmakers
oppose it.
Single-payer advocates point out that the United States is the only advanced nation without universal health care, which is true. Germany, the Netherlands and Switzerland have achieved universal coverage and affordable health care with, essentially, more comprehensive and generous forms of Obamacare that require people to buy insurance, tightly regulate insurers and provide subsidies to the poor and middle class.
State and federal lawmakers are exploring ways to increase coverage and lower costs. For example, the Nevada Legislature passed a bill in June that would have allowed people who make too much money to qualify for Medicaid to buy into that program. The bill, which would have required a federal waiver, did not become law because Gov. Brian Sandoval, a Republican, vetoed it. But the idea has other backers. Senator Brian Schatz of Hawaii said on Tuesday that he would introduce a bill that would explicitly allow states to let people buy into Medicaid.
Another approach would be to let people buy into Medicare at some point before they become eligible for the program at age 65. Hillary Clinton proposed this during her presidential campaign. Congress could also provide more generous subsidies to help middle-class people buy insurance on Obamacare exchanges. At the state level, four million people would gain coverage if Florida, Georgia, Texas and the 16 other states that
Ms. Pelosi has said that some states could go even further by approving single-payer systems of their own. California, Colorado, New York and Vermont have considered such proposals in recent years. If one or two states moved in that direction, it could help demonstrate the feasibility of such an approach in much the same way that Romneycare in Massachusetts provided plausibility for Obamacare.
The Republican campaign to repeal Obamacare, for all its waste of time and energy, has at least gotten people to talk seriously about proposals to improve the health care system.
Article link: https://www.nytimes.com/2017/08/26/opinion/sunday/obamacare-universal-health-coverage.html?smid=tw-nytopinion&smtyp=cur

Tuesday, August 15, 2017
In July, Commonwealth Fund staff got some distance from American health care by visiting Israel and the occupied West Bank of Palestine for cross-national health care discussions. The trip involved meetings in Haifa and visits to health care facilities serving Israelis and Palestinians in Haifa, Jerusalem, and the West Bank. Civil strife at the Al-Aqsa Mosque in Jerusalem and elsewhere in the West Bank provided sobering background to our journey — and we got a chance to see firsthand the medical consequences of ethnic and political conflict when we spent a morning at the hospital that treats Palestinians injured in conflicts with Israelis.
The trip was truly a tale of two health care systems that live side by side and interdigitate only at the margins. Israel has one of the world’s highest-performing health systems as judged by national health statistics and health spending levels. It invests modestly in health care, spending about 7.3 percent of GDP in 2016 (compared to an Organization for Economic Cooperation and Development (OECD) median of 9 percent). But it has population health statistics that are as good or better than OECD norms: a 2015 infant mortality rate of 3.1 deaths per 1,000 births, and life expectancy at birth of 80.1 years for men and 84.1 years for women in 2015.
The country’s excellent health results owe a great deal to a system that provides universal health care coverage and prioritizes primary care. Israelis admitted that they consider their hospital care only average in quality by international standards. All Israelis must enroll in one of four HMO-like health plans that pay for all services and directly provide most through a network of clinics and hospitals. We visited one primary care facility in Haifa — owned by Clalit, the largest health plan which enrolls about half the Israeli population. The clinic resembled the community health centers or equivalents that many of us have visited — and worked in — throughout the U.S. and elsewhere in the developed world.
We had conversations with staff from Clalit and other health plans about their use of case managers, social workers, and other health care personnel for managing high-need, high-cost members. Consistent with their universal use of electronic health records and other digital tools, the Israelis described their mostly successful efforts at health information exchange, and their work to develop predictive algorithms to help prevent and manage complex health problems. We came away feeling that we had a lot to learn from the Israelis — and they from us — about optimal approaches to organizing complex care and, especially, the use of digital tools to enhance care generally. Israel is a young, highly entrepreneurial, flexible, and pragmatic country. Its health care system runs lean, and this creates an appetite and aptitude for innovation.
We spent the last day and a half of the trip in and around Jerusalem, where we got an introduction to the Palestinian health care system. To say the least, this system does not have the resources or results of its Israeli counterpart. Spending was USD 294 per Palestinian in 2012 (compared to USD 2,046 per Israeli in 2011). Life expectancy at birth in 2015 was 70.7 years for men and 74.7 years for women, and infant mortality in 2014 was 12.6 deaths per 1,000 live births. The system is hampered by shortages of funding, personnel, and medications and by the pervasive poverty in occupied territories. Restrictions on movement in the occupied territories are also a huge problem for patients and providers.
We visited the principal Palestinian referral center and teaching hospital, Al-Makassed, which is located on the Mount of Olives with a majestic view of Jerusalem. Created in 1968, the facility claims to offer a full range of specialty services, but the plant was modest, and as described to us, funding is unpredictable. It depends on support from the Palestinian Authority — which is perennially in financial crisis — and aid from a variety of nongovernmental sources. Travel restrictions in the West Bank negatively affect health care access by the hospital’s patients, who must get permits from Israeli authorities before they can travel to East Jerusalem. Since Al-Makassed is also the primary source of specialty care for Gaza, access can be a huge challenge for residents of that isolated enclave. We were told that medical staff also frequently face long commutes through many checkpoints to reach the facility — and some have been banned entirely from entering East Jerusalem because of Israeli security concerns.
While we were visiting, the hospital was caring for injured Palestinians who had just clashed with Israeli riot-control forces. One of those patients died the next day.
We also spent a morning with the Israeli branch of Physicians for Human Rights, which organizes trips by volunteer Israeli health professionals to the West Bank and Gaza to provide health services. The visits take place once a week on Saturday mornings, so the group can minister to only 50 villages annually. Physicians for Human Rights has a waiting list of dozens of sites.
My colleague, Eric Schneider, and I had a chance as physicians to sit in on several health care encounters alongside one of the Israeli physician volunteers. We saw one family in which a young son had a previously corrected congenital heart defect (the surgery was in Israel) — but had had no follow-up in years — and the father carried a diagnosis of a rare autoimmune condition known as giant cell arteritis that was being treated with several very toxic medications, again with little continuity of care. The big challenge at this point — so familiar to anyone who has practiced in the United States — was paying for the additional care they needed, since they lacked health care coverage. And this family had the further challenge of getting permits to be seen either in East Jerusalem or, if necessary, in Israel.
There was no avoiding the conclusion that Palestinian health care is vastly inferior to the Israelis’, or that politics is a pervasive influence in the Israeli and Palestinian health care systems. Of course, the last six months have shown that politics is a huge influence on the U.S. health care system as well. The ethnic and income divides that animate U.S. health care politics are better concealed than the Israeli and Palestinian versions, but they are just as important. Our visit was instructive on many levels.
Article link: http://www.commonwealthfund.org/publications/blog/2017/aug/health-system-israel-palestine
A new survey finds a majority of physicians now support a single-payer health care system.

A July 2017 protest against the Republican health care bill in Milwaukee, Wisconsin. (Joe Brusky/Flickr cc 2.0)
This post first appeared at Kaiser Health News.
Single-payer health care is still a controversial idea in the US, but a majority of physicians are moving to support it, a new survey finds.
Fifty-six percent of doctors registered either strong support or were somewhat supportive of a single-payer health system, according to the survey by Merritt Hawkins, a physician recruitment firm. In its 2008 survey, opinions ran the opposite way — 58 percent opposed single-payer. What’s changed?
Physicians long for the relative clarity and simplicity of single-payer.
— Phillip Miller, vice president at physician recruitment firm Merritt Hawkins
Red tape, doctors tell Merritt Hawkins. Phillip Miller, the firm’s vice president of communications, said that in the thousands of conversations its employees have with doctors each year, physicians often say they are tired of dealing with billing and paperwork, which takes time away from patients.
“Physicians long for the relative clarity and simplicity of single-payer. In their minds, it would create less distractions, taking care of patients — not reimbursement,” Miller said.
In a single-payer system, a public entity, such as the government, would pay all the medical bills for a certain population, rather than insurance companies doing that work.
A long-term trend away from physicians owning their practices may be another reason that single-payer is winning some over. Last year was the first in which fewer than half of practicing physicians owned their practice — 47.1 percent — according to the American Medical Association’s surveys in 2012, 2014 and 2016. Many doctors are today employed by hospitals or health care institutions, rather than working for themselves in traditional solo or small-group private practices. Those doctors might be less invested in who pays the invoices, Miller said.
There’s also a growing sense of inevitability, Miller said, as more doctors assume single-payer is on the horizon.
“I would say there is a sense of frustration, a sense of maybe resignation that we’re moving in that direction, let’s go there and get it over with,” he said.
Merritt Hawkins emailed its survey August 3 and received responses from 1,003 doctors. The margin of sampling error is plus or minus 3.1 percentage points.
RELATED: Health & Science
The Affordable Care Act established the principle that everyone deserves health coverage, said Shawn Martin, senior vice president for advocacy at the American Academy of Family Physicians. Inside the medical profession, the conversation has changed to how best to provide universal coverage, he said.
“That’s the debate we’re moving into, that’s why you’re seeing a renewed interest in single-payer,” Martin said.
Dr. Steven Schroeder, who chaired a national commission in 2013 that studied how physicians are paid, said the attitude of medical students is also shifting.
Schroeder has taught medicine at the University of California-San Francisco Medical Center since 1971 and has noticed students’ increasing support for a single-payer system, an attitude they likely carry into their professional careers.
“Most of the medical students here don’t understand why the rest of the country doesn’t support it,” said Schroeder.
The Merritt Hawkins findings follow two similar surveys this year.
In February, a LinkedIn survey of 500 doctors found that 48 percent supported a “Medicare for all” type of system, and 32 percent opposed the idea.
The second, released by the Chicago Medical Society in June, reported that 56 percent of doctors in that area picked single-payer as the “best care to the greatest number of people.” More than 1,000 doctors were surveyed.
Since June 2016, more than 2,500 doctors have endorsed a proposal published in the American Journal of Public Health calling for single-payer to replace the Affordable Care Act. The plan was drafted by the Physicians for a National Health Program (PNHP), which says it represents 21,600 doctors, medical students and health professionals who support single-payer.
Clare Fauke, a communications specialist for the organization, said the group added 1,065 members in the past year and membership is now the highest since PNHP began in 1987.
Kaiser Health News, a nonprofit health newsroom whose stories appear in news outlets nationwide, is an editorially independent part of the Kaiser Family Foundation.
Article link: http://billmoyers.com/story/doctors-accept-single-payer-healthcare/
