A proposed Centers for Medicare and Medicaid Services rule that would mandate data sharing for organizations participating in the program has split the industry into a wide debate that questions what’s needed to get healthcare providers to share necessary patient information.
Proposed in April, the proposed rule would mandate providers share patients’ discharge information and other relevant information as part of the conditions of participation. Stakeholders had until June 26 to give feedback on the proposal, and there are a wide range of supporters and protestors on both sides of the argument.
Unhappy stakeholders
The American Hospital Association is staunchly against the proposed rule and is concerned about how compliance would be measured. The group also highlighted the difficulties in sharing medical data with post-acute providers.
AHA officials said those groups weren’t provided the resources or incentives to adopt health IT and the “requirement would put another unfunded mandate on these organizations.”
“Such a requirement would only be workable if all facilities were afforded the same opportunity to acquire certified EHRs that actually conformed to standards that enable the kind of interoperability CMS envisions,” the group wrote.
[Also: Next-gen interoperability: AI, blockchain, FHIR and open source analytics]
CHIME officials said CMS is taking the wrong approach: “Simply imposing regulatory requirements that make electronic data exchange a condition for providers to receive Medicare payment does not address the root issues at play.”
Instead, CMS needs to address the ongoing challenges surrounding interoperability, and “importantly too, a distinction must be drawn between speeding and increasing data exchange among providers and achieving a true state of interoperability. The two should not be conflated.”
The Electronic Health Record Association echoed those opinions, and officials said that CMS first needs to address information blocking and wait for the 21st Century Cures mandates are complete.
“It is additionally unclear how interoperability expectations in the conditions of participation would be evaluated and audited, but it seems likely that evaluation and auditing of these items would generate additional hospital burden.”
Also opposing the rule was the American Medical Informatics Association, which sent in 38 pages of comments. Although the group is “generally supportive of the balance envisioned” by the rule, officials wonder whether the proposed standard would actually help information blocking.
AMIA officials said they think that providers do want to share information, but it “isn’t occurring consistently.” As a result, CMS should first handle the information blocking rule before it modifies the conditions of participation.
“We recommend CMS focus its inquiry on provider-to-patient information flows and calibrate its policies to ensure that all entities receiving Medicare funds provide patients 24x7x365 access to their information in a persistent manner and without special effort,” the group wrote.
“We find the concept of ‘medically necessary information’ somewhat abstract and very context-dependent,” they added.
Those in favor
Those in support of the rule argued that the technology makes data sharing possible and enforcing data sharing as a condition of participation will force providers to improve care coordination.
HIMSS was among the supporters that feel CMS should explore “all available policy levers to promote interoperability,” and those include revising the conditions of participation. Further, officials suggested CMS modify the Trusted Exchange Framework and Common Agreement to help organizations meet those requirements.
A group of 50 organizations, including ACOs, health information exchanges, Intel, Beth Israel Deaconess and others sent a letter, voiced support of the proposed rule, calling on CMS to more aggressively promote interoperability and health information exchange.
“Now is the moment for a focused and rigorous effort to liberate the data currently available in the healthcare system to enable patients and their providers seamlessly access and share all their digital health information,” the groups wrote.
“We believe the time is right to move past the current rigid and siloed system into one prepared to take advantage of all the opportunities made available in our digital age,” they continued.
The supporters also said the data sharing policy would be a tremendous benefit to millions of patients and stressed that discharged information should not only be required, but share within 24-hours. But the groups said that it’s important for CMS to allow providers to meet those requirements over time.
CMS plans to review all provided stakeholder comments when it develops its regulatory proposals and guidance.
Article link: https://www.healthcareitnews.com/news/proposed-cms-interoperability-requirements-split-industry-groups
Twitter: @JessieFDavis
Email the writer: jessica.davis@himssmedia.com
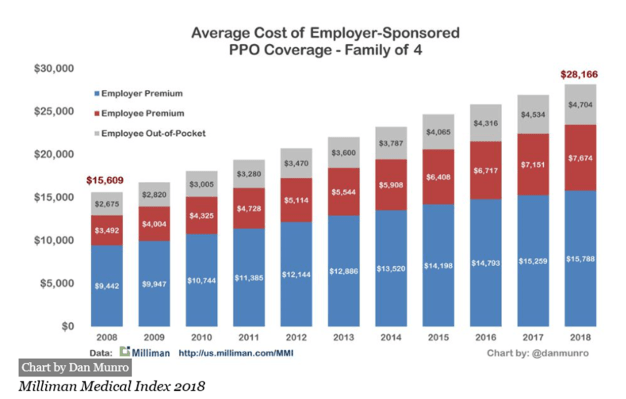
 Survey shows only about half of Americans would have money to pay for an unexpected medical bill of $1000.
Survey shows only about half of Americans would have money to pay for an unexpected medical bill of $1000.