When you walk into the Arlington Women’s Center, you see a spacious waiting room with artwork on the wall, maroon chairs, and a friendly receptionist sitting at the front desk.
When you walk into the Arlington Women’s Center, you see a spacious waiting room with artwork on the wall, maroon chairs, and a friendly receptionist sitting at the front desk.
The obstetrics and gynecology practice serves a high-income suburb of Washington, DC. Framed photographs on the wall advertise the center’s physicians who’ve made lists of the city’s best doctors. It’s a modern, upscale doctor office.
Listen to the podcast version of this story: It’s time to face the fax
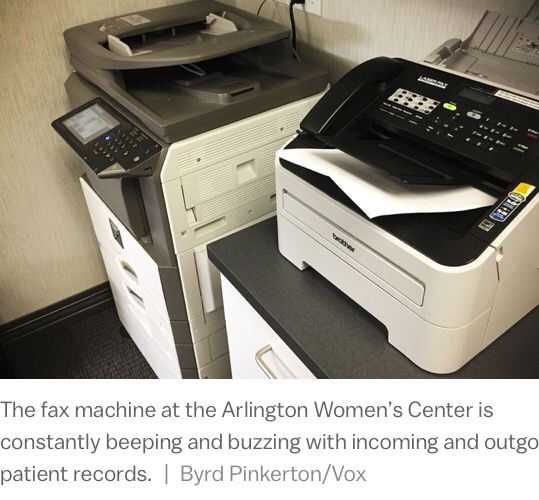
But when it needs to share patient records, it turns to an outdated technology: the fax machine.
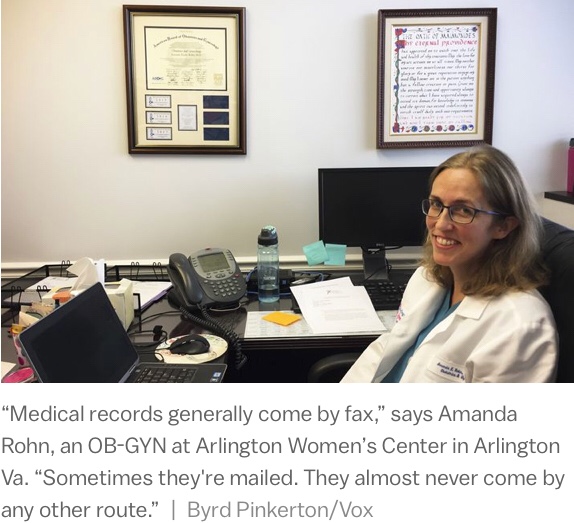
“The pages get jammed up so you end up with half-pages that come out at the other end,” says Amanda Rohn, an OB-GYN at Arlington Women’s Center, “or you get blank pages that don’t actually have the information you need.”
The clinic has digitized its own patient data. But its electronic system can’t connect with other clinics’ records. So when doctors want to retrieve records from another office — an ultrasound for a pregnant patient, for example — they have to turn to the fax.
Most women at the Arlington Women’s Center get their ultrasounds at a radiology office that is in the same building, just a floor below. It also has a digital record. But the two systems don’t connect. So they use a Rube Goldberg-esque analog method for sharing data: Print out pages of one record, fax it, and then scan those pages into the other digital system.
“We have a medical records department who goes through all the incoming faxes, sorts them for which doctor they go to, and then I have a folder where they put my results in,” Rohn says, pointing to a pink file folder on her desk. “If we were all on the same system, I’d be able to see everybody’s results, but since we’re not, there has to be some way they get to me.”
Most industries abandoned the fax machine in the 1990s, and for good reason. Fax machines are terrible at sending data. Busy signals interfere. Printouts are blurry. And sometimes faxes go to the wrong place entirely.
One medical worker recalled a fax fiasco from the 1990s when he practically sent medical records to the moon. “The FBI called about a half-hour later and asked how I got the number,” he said. “I told them that I was faxing Minnesota. They told me I had faxed NASA.”
In the medical sector, the fax is as dominant as ever. It is the cockroach of American medicine: hated by doctors and medical professionals but able to survive — even thrive — in a hostile environment. By one private firm’s estimate, the fax accounts for about 75 percent of all medical communication. It frustrates doctors, nurses, researchers, and entire hospitals, but a solution is evasive.
At Rohn’s obstetrics practice, no one has contacted NASA by mistake, but they’ve had real problems. Lately, doctors have taken to hand-delivering the most important records.
“We used to fax the labor and delivery records, but they didn’t get them or they were misplacing them,” says Hilda Moreno, who manages the office’s medical records. “We kept getting calls like, did you send this? And we’d say we did. So we started printing them out.”
Obama tried to force the health sector to go digital. But he didn’t make the systems talk.
The story of the fax machine’s dominant role in medicine is also the story of a government incentive program that badly misread the economics of American health care.
The Obama administration spent upward of $30 billion encouraging American hospitals and doctor offices to switch from paper to electronic records. The program was a wild success, in one respect. The number of hospitals using electronic records grew from 9 percent in 2008 to 83 percent in 2015, a huge change in less than a decade.
But the program didn’t account for a critical need: sharing. Hospital and doctor offices generally remain unable to transfer electronic information to other hospitals and doctor offices. Billions of dollars later, they are left printing out documents and faxing them. And so the fax machine remains medicine’s dominant method of communication.
“MEDICAL RECORDS GENERALLY COME BY FAX. SOMETIMES THEY’RE MAILED. THEY ALMOST NEVER COME BY ANY OTHER ROUTE.”
Obama officials believed competing health systems would volunteer to share patient data. They now admit that was naive.
“We don’t expect Amazon and Walmart to share background on their customers, but we do expect competing hospital system to do so,” says David Blumenthal, who coordinated health policy for the Obama administration from 2011 to 2013. “Those institutions consider that data proprietary and an important business asset. We should never have expected it to occur naturally, that these organizations would readily adopt information exchange.”
The stimulus package that President Obama signed into law in February 2009 included a 53-page section called the HITECH Act (an acronym for its much clunkier full name: the Health Information Technology for Economic and Clinical Health).
The small part of the massive stimulus bill included more than $30 billion to spend incentivizing doctors to adopt digital records. The law directed a small, little-known government agency — the Office of the National Coordinator for Health Information Technology (ONC) — to develop a program to distribute the money.
“It was quite small and had modest operational responsibilities,” says Blumenthal.
The agency historically subsisted on a meager budget with a few dozen staffers. All of a sudden, it had a multibillion-dollar budget and pressure from the White House to spend that money quickly. The Obama administration hoped this infusion of money would help drag the country out of the 2008 recession.
“The White House looked at these billions of dollars and they saw an opportunity to stimulate the economy,” Blumenthal says. “We did have pressure from the White House to get the money out the door.”
Blumenthal’s team had to move quickly, and decided to focus on getting doctors to adopt electronic records. Once doctors started using electronic records, the thinking at the time went, they would naturally start using more digital forms of communication like secure email.
“Our philosophy was, you’ve got to have the information in bits and bytes before you can start sending those down the internet to someplace else,” Blumenthal says.
Farzad Mostashari, who took over Blumenthal’s position in 2013, recalls the ambitions similarly. “The real goal at the time was, hey, let’s get folks off of paper and onto electronic health records,” he says.
ONC came up with “meaningful use” standards, a checklist of benchmarks that doctor and hospital offices would need to hit in order to receive a small slice of that $30 billion incentive fund. If doctors and hospitals were able to meet these criteria, they’d get bonus payments from the federal government.
All available data suggests that the meaningful use incentives hugely increased the adoption of electronic medical records. A recent paper in the journal Health Affairs compared the adoption of digital records among hospitals (which qualified for these incentive payments) and nursing homes (which didn’t get the bonuses).
It found that the facilities eligible for the bonus payments adopted digital records at a much faster pace than those without much incentive.
“We now have data to suggest the majority of electronic health record adoption was because of the HITECH Act,” says Julia Adler-Milstein, the lead author of that study and an associate professor at the University of California San Francisco School of Medicine. “We would not have seen those double-digit percentage point increases without it.”
If you can now log in to a patient portal at your doctors’ office to schedule a visit, see results of a test, or send a message to your physician, that is likely the result of the HITECH Act.
But if you’ve ever become frustrated trying to get one doctor to talk to another, that is the Obama administration’s legacy too.
“The fax machine is still a major part of medical communication”
Rohn works on that Virginia hospital campus I mentioned earlier. And for years, she’s had a front-row seat to the Obama administration’s struggle to digitize American medicine.
The 36-year-old received an undergraduate degree in engineering and initially planned to pursue a career in programming. “It turned out that I didn’t like spending all my time looking at a computer screen,” she said. “I really wanted to spend my time interacting more directly with people.”
Rohn went back to medical school and in 2013 completed a residency in obstetrics and gynecology at the University of Pennsylvania. She began cold-calling OB-GYN practices that had openings in the DC area, where her husband already had a job.
Office after office told her the same thing: Stop calling us. Just fax us your résumé.
“The fax machine is still a major part of medical communication,” she says. “It’s crazy that I was sending my CV by fax machine in 2013.”
Rohn began sending unsolicited faxes with her résumé to OB-GYN practices, and, amazingly, it worked. One of her faxes went to Arlington Women’s Center, where she works today.
When Rohn was a resident, she used a lot more paper records. When she saw patients in the hospital after surgery or a delivery, she would handwrite notes in a paper chart.
She started her job just as billions of federal incentive dollars were flowing to get doctors to switch to digital records. Her clinic digitized just before her arrival in 2013. Now, instead of scribbling patient notes in handwriting, she types them into her electronic record.
She can order most lab results through the electronic record, too, after a lengthy effort to connect her office’s digital system with the laboratory they work with most frequently.
“I can see each encounter the patient has had in our clinic, so I can look back and see when my colleague saw this patient last year, read her notes, know what they talk about,” Rohn says.
It’s when she wants to communicate with other offices that things get tricky. The hospital where most of her patients deliver uses Epic, the medical records company with the largest market share in the United States. Rohn’s office uses a smaller company called NextGen.
Each day, Rohn comes into the office to a pink folder on her desk labeled “prenatal labs” that contains a stack of faxes from other offices she needs to enter into the electronic record.
When Rohn’s patients are close to giving birth, at 36 weeks pregnant, she or another doctor hand-delivers their medical records to the labor and delivery department. It’s not a great system.
“Sometimes we can’t find the records because someone has misfiled it or someone never sent it,” Rohn says. “Or they’re not that far along yet in pregnancy if they deliver prematurely.”
Rohn is a highly trained professional. She spent four years at top-ranked medical school and more years after that as a resident learning how to deliver babies, perform surgeries, and help patients through pregnancy.
But because of America’s disconnected medical system, she spends a significant amount of time transcribing medical records and hand-delivering them around her hospital. This is time when she could be using her medical expertise to see more patients or have longer visits. Instead, she’s managing paperwork.
And this wastes her patients’ time too. Sometimes Rohn will have appointments to discuss an abnormal Pap smear but won’t be sent the actual results that show what is abnormal.
“So then I’m seeing someone in consultation for abnormal Pap smear and I don’t know what result was, and we have to decide do we do the test again today when you might not actually need it,” she says.
There are financial incentives to keep using the fax machine
It turns out there are strong economic incentives for doctors to keep patient information to themselves — and even stronger incentives for electronic medical records not to play nicely with each other.
While patients might want one hospital to exchange information with another hospital, those institutions have little incentive to do so. A shared medical record, after all, makes it easier to see a different doctor. A walled garden — where records only get traded within one hospital system — can encourage patients to stick with those providers.
“When you want competing entities to share information, you have to realize that they’re sharing things that could help their competitors,” says Blumenthal.
The program that Blumenthal helped build required hospitals to have the ability to share information, but it didn’t mandate that they do so frequently or make the process especially easy. Most hospitals made a rational business decision and did not invest in technologies that would make it easier for competitors to siphon off patients.
Competitive pressure between the companies that sell electronic record makers themselves only made things worse. The electronic record makers don’t have much incentive to connect well with other records, when they’d rather just convert that hospital on a different electronic platform into one of their own customers.
“WHEN YOU WANT COMPETING ENTITIES TO SHARE INFORMATION, YOU HAVE TO REALIZE THAT THEY’RE SHARING THINGS THAT COULD HELP THEIR COMPETITORS”
“If [electronic record vendors] expended all that time and effort to make it so anyone could plug into any other system, it’s reducing the advantage of staying on your particular network,” Mostashari says.
This is especially true for larger electronic medical record companies, which want to sell the advantages of joining a record that is used in lots of doctor offices. “You want to make it easier for people to say, ‘Hey, if you’re on [our electronic record], look how awesome it is! You can talk to any user, anywhere in the country,” he argues.
In short, economics gave hospitals plenty of reasons not to connect their records with other hospitals — to stick with a clunky technology, like fax, that makes it hard to transmit information. And the government didn’t give any incentives to connect — it stopped at digitizing medicine, falling short of the interoperability that patients actually want.
How do you actually kill the fax machine?
Mostashari came away from his time in Washington believing a fix would require more government intervention — namely, outlawing faxing in American medicine. He argues that doctors won’t leave the fax until there is an expiration date, a moment when the government forces them to use secure email instead.
“I think if we want to kill the fax, we need to schedule a funeral,” he says. “I think you need a pull and you also need a push.”
The Trump administration, however, will take a different approach. Donald Rucker now runs the Office of the National Coordinator for Health Information Technology, and did not take kindly to the federal mandate proposal.
“All of the thousands of regulations that have piled on have the net effect of preventing us as individuals from controlling our data, from shopping for care, or having vaguely cost-effective care to shop for,” Rucker said.
He argues that better-designed electronic records will go a long way toward allowing data to transfer more freely. He also cited a new provision in a recent health care law, the 21st Century Cures Act, that requires electronic records to exchange data with other records in a way that requires “no special effort.” What “no special effort” means isn’t yet clear, and will likely be defined in future regulations.
“I THINK IF WE WANT TO KILL THE FAX, WE NEED TO SCHEDULE A FUNERAL”
The verdict is still out on whether the Trump administration’s approach can work — or whether, eventually, a more heavy-handed mandate will be needed to actually kill the fax.
But we do know this: As long as the fax sticks around, it is bad for doctors and bad for patients.
Article link: https://www.vox.com/health-care/2017/10/30/16228054/american-medical-system-fax-machines-why
 WASHINGTON — The Department of Veterans Affairs is preparing to shift billions of dollars from government-run veterans’ hospitals to private health care providers, setting the stage for the biggest transformation of the veterans’ medical system in a generation.
WASHINGTON — The Department of Veterans Affairs is preparing to shift billions of dollars from government-run veterans’ hospitals to private health care providers, setting the stage for the biggest transformation of the veterans’ medical system in a generation.