On Tuesday, the House Veterans Affairs Committee held a legislative hearing on a number of bills, including H.R. 2123, the Veterans E-Health and Telemedicine Support Act of 2017. This bill would improve the ability of healthcare professionals to treat veterans through the use of telemedicine by addressing state licensure issues. At the hearing, both witnesses and Members of Congress praised the VA’s use of telehealth, touting the many benefits that telehealth provides to veterans. However, they also acknowledged that current limitations and questions around the practice of telehealth across state lines is problematic for healthcare professionals within the VA, and hoped that the bill would address these concerns. At the hearing, they also touched upon the VA’s transition from VistA to a Cerner EHR system in order to become more interoperable with the Department of Defense. Secretary David Shulkin stated that it could take 18 months for its first site to go live with the new EHR system, and around seven to eight years to fully transition.
Also on Tuesday, the House Homeland Security Subcommittee on Cybersecurity and Infrastructure Protection and the House Committee on Education and the Workforce Subcommittee on Higher Education and Workforce Development held a joint hearing entitled “Public-Private Solutions to Educating a Cyber Workforce.” The hearing featured witnesses from academia, the private industry and the nonprofit sector and focused on ways the government and private sector can work together to address the growing demand for cybersecurity professionals across all sectors of the economy. During the hearing, both Members of Congress and witnesses highlighted that our education system is not producing the number of qualified cybersecurity professionals to meet ever growing demand. Addressing the shortage of qualified cybersecurity professionals is a key priority for HIMSS and several recommendations for addressing the shortage can be found in HIMSS Cybersecurity Call to Action.
On Wednesday, the House Energy and Commerce Subcommittee on Communications & Technology held a hearing on Oversight of the Federal Communications Commission, featuring all five FCC Commissioners as witnesses. During the hearing, commissioners and Members of Congress expressed support for rural broadband deployment, telehealth and remote patient monitoring. Rural broadband deployment is a key priority for HIMSS and is addressed in HIMSS 2017 Infrastructure Congressional Ask
Provider identity management could be the ideal case study for proving blockchain can generate trust between payers and providers for value-based care.
– As the healthcare industry slowly becomes more connected and more interoperable, organizations are attempting to implement data management strategies that balance privacy and security with collective access and accessibility.
Value-based care has accelerated the need for seamless data sharing in an environment that is both transparent and unquestionably trustworthy – one that can bring payers and providers together to improve quality, reduce costs, and enhance the patient experience.
While stakeholders have offered up plenty of potential solutions for creating a free-flowing data environment that can support the complex environment of pay-for-performance reimbursements, blockchain may be the methodology that ticks the most boxes with a relatively low amount of effort.
At Hashed Health, an industry consortium dedicated to applying blockchain to real-world use cases, CEO John Bass believes that the distributed ledger approach offers a number of promising improvements to the way providers, payers, and patients collaborate in a value-based world.
Like many innovative technologies, however, blockchain has been subject to skepticism about its possible role in the health data exchange ecosystem.
Surveys and reports have suggested that providers, payers, and pharmaceutical companies are among the stakeholders eager to explore blockchain-based tools for administrative tasks, data exchange, and patient management.
John Bass, CEO of Hashed Health Source: Xtelligent Media
Yet only a handful of developers are starting to offer healthcare-focused products, and few concrete case studies have emerged to show that the strategy really works at scale.
“Everyone is very excited about the disruptive potential of blockchain, but we don’t want to get lost in the hype,” acknowledged Bass.
“If we want to prove it can make a real difference, we need to anchor the industry with some simple demonstrations of value.”
For Hashed Health, the often overlooked issue of provider identity and reputation management is the perfect gateway project for blockchain.
Ensuring that physicians, nurses, pharmacists, and other clinicians are correctly licensed and credentialed to provide specific services is a foundation for all payment from health plans, whether the reimbursement is fee-for-service or pay-for-performance.
“It might not be the juiciest use case, but it’s something that everyone in the industry is looking to improve,” Bass noted. “It’s a good starting place because the information involved isn’t overly sensitive. It isn’t a politically charged issue, and there aren’t a lot of existing competitive interests.”
“Everyone is searching for a better solution to a shared problem, which makes it a perfect place to innovate with low barriers to entry for those who want to try new strategies.”
Currently, validating and verifying a physician license is very much a manual process. Phone calls, faxes, and emails are the primary method of communication, taking up time and causing confusion if a critical piece of information is somehow lost in transmission.
And with the introduction of the Interstate Medical Licensure Compact, which offers a pathway for licensure reciprocity across 22 states, the process is ripe for attention.
“There is no real system to enable the sharing of that information across such a large number of stakeholders right now,” Bass said. “We believe that blockchain offers a clear value proposition for them.”
“The participating states could build a centralized database managed by some for-profit or non-profit company, and worry about trying to secure funding for that indefinitely,” he said. “Or they could try to create a decentralized network that requires much less ongoing expense while offering a trusted and easily validated way of managing identities across states and regions.”
Blockchain can provide the framework required to support cross-state information exchange, he asserted.
“An individual can put a certificate of attestation of licensure on the blockchain and other states are able to see that on the network,” Bass explained. “That offers a faster, better, cheaper way to ensure that everyone remains up-to-date without all the back-and-forth of traditional communication.
Hashed Health is already working with the state of Illinois to put the concept into action. A pilot project, announced in August, aims to prevent bottlenecks in the licensure process and offer a more secure and streamlined way to manage this necessary dataset.
If the initiative is successful, it could result in more confidence that blockchain is ready for prime time in healthcare. Wider adoption for identity management could expand into leveraging distributed ledger technology for other key value-based care tasks.
“Provider identity is an important tie-in to value-based care and contextual payments,” said Bass. “Value-based reimbursement is about the relationship between cost and quality. In a perfect world, we could use blockchain create a value exchange that would take both of those into account – and make sure that the person who is earning the payment is qualified and validated to do so.”
At the moment, cost and quality calculations are separated by a layer of administrative action. Payers must accept, adjudicate, and analyze claims data and provider quality reporting results before they can decide whether to disburse an incentive payment or withhold a penalty.
“Blockchain is one of the emerging technologies that would allow payers to programmatically throttle payments or incentives based on external data sources instead of adjusting payments through laborious administrative processes,” said Bass.
“As long as you can provide an attestation that a certain best practice is being followed, you can create credits and debits in the provider’s virtual wallet to provide incentives. That is a fundamental redesign of what value transfers look like today.”
Placing a certificate of provider identity on the blockchain could form the foundation for a series of future blockchain breakthroughs that simplify the administrative processes involved in a successful value-based care contract.
Hashed Health is working concurrently on a number of interconnected projects, including blockchain approaches to managing patient identities, clinical trial data, Internet of Things devices, and aspects of the healthcare supply chain.
As the consortium grows, Bass is anticipating that the organization’s members will continue to develop innovative use cases and value-driven products with a variety of blockchain technologies at their core.
Developers are currently using many of the emerging standards frameworks to create their offerings, including Tendermint, Hyperledger Fabric 1.0, and Etherium.
“We are continually searching and testing our technical and our business assumptions to make sure that we have the right long-term solution,” Bass said.
“We know we’re moving in the right direction with these value-based data exchange concepts. We think blockchain and its programmable value characteristics have the ability to change the conversation and start building momentum for the industry to adopt distributed ledger tools.”
Back in the 90s, consider the thought of someone telling you, “If you sit in front of this screen beside a humming box, you can access other people all over the world that are sitting in front of screens beside humming boxes.”
(I’m talking about computers.)
Most people didn’t believe it. In fact, they couldn’t fathom the idea of Internet, let alone warrant spending the money on something that had so few people (generally speaking) having bought into the idea. The Internet back then was more of a small town than a world wide web.
Then more people started to hear about it. They would log online, experience the feeling of connecting with someone online, and immediately tell someone else. As a result, the Internet started to grow exponentially–as both a social idea, and as a transformative way of expanding or even building a business.
Before long, the dot-com boom was in full effect, and it was clear the Internet was no longer “just an idea.” It truly was set to change the way human beings communicate here on earth.
That was step one.
We forget that two decades ago, it was rare for someone to have a computer in their home–whereas today, we tilt our heads in confusion at anyone who doesn’t own a computer. And a huge part of society’s adoption of the Internet has been reliant upon the improvement of technology. The Internet, purely as a concept, probably lived in the heads of brilliant dreamers and innovators long before it actually came to fruition. It was the technology we were waiting on, and as technology as scaled and improved, so too has the idea of global connectivity.
Today, we are witnessing that same process happen again with blockchain technology.
If it’s taken us two decades just to get computers and Internet access to the global population (and keep in mind, we’re still only halfway there–only 51% of the world is on the Internet), then the next logical step is going to be solving for how to make better use of all those idle resources.
That’s one of the biggest issues blockchain tech is working to solve. Why build one (centralized) solution that can be used (and/or bought) by everyone, when you can leverage the power of Internet users with computers to make everyday resources more effective?
Here are 3 very clear examples:
1. Utilizing blockchain tech to rent your unused bandwidth.
Developers, designers, engineers and “big idea” entrepreneurs have worked hard to make the Internet as easy to use as possible for everyday consumers. But behind that strategically simple Google page is a whole lot of back-end jargon most people don’t understand.
A prime case-in-point is when a webpage goes down. Internet users will sit there hitting refresh wondering why it’s not working, with no real insight into why. And on the flip-side, businesses spend exorbitant amounts of money protecting against DDoS attacks, malware, and other intrusions that disrupt service or compromise user data.
Thinking conventionally, the Internet has always viewed this problem as something solvable by a private provider. But when put in the context of blockchain, why hire one company or use one software tool to help protect against DDoS attacks when you can leverage the spare network bandwidth of other Internet users? Combined, that decentralized web is far more powerful.
Gladius, a blockchain platform, is already working on making this back-end solution mainstream, allowing everyday users to rent out their bandwidth–and earn tokens (which can be converted into currency) in return.
This is the same sharing economy model we have seen explode in popularity over the past few years–Uber, Airbnb, etc.–except in a more tech-heavy form.
2. Monetizing your hard disk space.
Building off the Uber and shared economy example above, think about how people’s perspectives have changed in the past few years in terms of how they rationalize buying a car, or even an apartment.
We now think, “Sure, this might be expensive, but I can offset the cost by renting it out a few days a month.”
The exact same thing is happening with computers and everyday users who have available storage on their computers. Filecoin is a blockchain platform that believes it’s far better to host the Internet’s vast library of information across a variety of different points–rather than keeping huge libraries of data in any one central location. And some of Silicon Valley’s most prolific investors seem to agree.
According to Techcrunch, in August, 2017, Filecoin closed out their “advisor” sale, raising $52M from 150+ investors, including Sequoia Capital, Andreessen Horowitz, Union Square Ventures, and Winklevoss Capital, among others. If that’s not reason enough to give the idea of sharing your hard disk space some serious thought, Filecoin’s ICO in September raised a jaw-dropping $205.8 million.
3. Monetizing idle computing power
Similar to renting hard disk space, what about your computer’s power? Can’t that be shared as well?
Most people, when using their computers, only use a small portion of their computing power–similar to someone driving a sports car below the speed limit.
Golem is a blockchain platform is working to make the power of a supercomputer available to everyday users by combining computing power into one decentralized network. According to Forbes, “The Golem Network, in its role as an Airbnb for computing-processing power, enables machines around the world to transact with each other.”
The idea here is, instead of each individual consumer working to buy the most powerful machine out there in order to compute heavy sets of information, Golem users can tap into that same power in a decentralized and more affordable way.
When you look at these different use cases for blockchain, it’s clear that where we’re headed in terms of innovation is absolutely within a shared economy. Sharing hard disk space, sharing computing power, sharing resources in a way that benefits both the individual user and the collective whole, both in terms of efficiency, but also transparency and safety.
The opinions expressed here by Inc.com columnists are their own, not those of Inc.com.
Michael J. Casey is the chairman of CoinDesk’s advisory board and a senior advisor for blockchain research at MIT’s Digital Currency Initiative.
In this opinion piece, one of a weekly series of columns, Casey looks at how blockchain might free society from the stranglehold of the four giant data hogs of the internet era: Google, Amazon, Facebook and Apple.
What’s wrong with this picture
The front page of The Wall Street Journal, Tuesday: “Amazon Lures 238 Bids for its Second Home.”
It’s not a good thing that a single company can get the political leaders of so many American cities and states to scramble over each other to try to lure $5 billion in spending on some new buildings.
The story shows that Amazon’s influence over American urban life is far more than one company deserves: over tax policies, over city planning decisions, over the aesthetics and culture of our communities. Society’s interests lie in sustaining a dynamic, innovative and evolving economy, not one in which hegemonic companies have oversized sway over everyone’s decision-making.
This is the core problem of centralization in the internet age – a pet topic for those of us who believe the ideas behind blockchain technology can point us toward a better economic model.
Amazon is not alone, of course. But it’s in a very select group. An acronym has emerged to define the small club of digital behemoths to which it belongs: GAFA (Google, Amazon, Facebook and Apple).
Two other WSJ stories this past week bring home the distorting influence of two other members of that club. One was Christopher Mims’ column about Facebook’s “master algorithm,” which in determining what we see and read is literally dictating how we think. The other was about Google winning the quantum computing race, a prize that will afford the winner unimaginable competitive advantages in data-processing capabilities.
Meanwhile, with my iPhone 6’s screen cracked and its functionality deteriorated since I upgraded to iOS 11, I’m tempted to switch to a Samsung phone, but don’t want to lose all the data and connectivity that the Apple universe has locked me into. And I know that with the Android OS, I’d just be getting Google’s version of the same dependency anyway.
The internet’s original sin
How did the GAFA gang get to be so powerful? It comes down to an original sin in the first design of the internet.
The inventors of packet switching and of the basic protocols on which the modern web is built did a masterful job figuring how to move information seamlessly across a distributed network. What they didn’t do was resolve the problem of trust.
Since information is power, it is often highly sensitive. So when people share it with each other, they need to know that data can be trusted. But since there was no truly decentralized trust mediation system in place in the 1990s – no permissionless way to solve the Byzantine Generals’ Problem – an asymmetric solution was found.
On the one hand, the distribution of public information was disintermediated, which put all centralized providers of that information, especially newspapers and other media outlets, under intense business pressure from blogs and other new information competitors. But on the other, all valuable information – particularly money itself, an especially valuable form of information – was still intermediated by trusted third parties.
It was a centralized solution bolted onto a decentralized information infrastructure.
So, we got website hosting services to manage each site’s files. We got certificate authorities to authenticate reliable addresses. We got banks and credit card providers to run the payment system. And since we craved the network that Facebook’s community offered and that Amazon’s marketplace could reach and Google’s search engine could tap, we fed ever more valuable information into the hands of these entities – those that won the early, defining battles to establish dominance of those services.
A new internet version of the trusted third party was born, and it was just as powerful, if not more so, than those archetypal trusted third parties of the pre-internet era: banks.
Only these newcomers’ currency isn’t dollars, it’s data.
A decentralized way forward
Lately, problems such as Facebook’s “fake news” dilemma and Equifax’s cyberbreach have finally begun shining a light on the fundamental flaws of a centralized system for controlling sensitive information. But our economy was suffering long before that as result of this re-intermediation.
Since producers now depend on Amazon to reach their customers, their entire business model – from production processes to their planning strategies – is determined by whatever information is generated by the Seattle company’s algorithm. That’s an inherent impediment to effective innovation and creates a dependency that limits competitive capabilities.
If you think this level of domination is bad, consider what will happen when we arrive at a world in which artificial intelligence, machine learning and the Internet of Things have combined to ensure that virtually every decision we make is automated by some algorithm. The question “who owns the data?” is going to become a much bigger problem.
I don’t know if the blockchain will ultimately solve all this. In the blockchain space, there are unsolved challenges relating to how to scale permissionless blockchains such as bitcoin, as well as questions about how much autonomy people want or should have over their own money and their data.
But surely the answer lies somewhere within the core concept of a decentralized trust mechanism that blockchain points to.
Within the model that Satoshi Nakamoto’s invention produced – a system for how to agree on the validity of information shared by strangers in an environment of mistrust – we have a new framework for thinking about who gets to manage data in the internet age.
The idea that the global economy of the future will be one in which individuals and small businesses have direct control over their data, and yet can still operate in open markets and generate network effects is an exciting prospect. It’s a future in which a more level playing field gives rise to true competition and unleashes the kind of open-source innovation that’s needed to solve many of the problems we face.
That world will eventually come. The places that win in that environment will be those that first embrace a new, decentralized model for data sharing and peer-to-peer trading that promotes true competition. The losers will likely include whichever city wins the 2017 beauty contest to host Amazon’s new headquarters.
The leader in blockchain news, CoinDesk strives to offer an open platform for dialogue and discussion on all things blockchain by encouraging contributed articles. As such, the opinions expressed in this article are the author’s own and do not necessarily reflect the view of CoinDesk.
The U.S. government agency in charge of logistics is taking the next step in its effort to better understand blockchain.
Through its Emerging Citizen Technology (ECT) program, a blockchain analysis effort first announced in September, the General Services Administration (GSA) this week opened to contributions from industry members, according to a post on its website.
These contributions will now be compiled into an open-source tool called Atlas, which will include “programs, use cases and resources” created by the private sector and researchers working within government agencies.
The ECT is meant to serve as a resource that clarifies the potential uses of blockchain technology, both for the U.S. government and for the general public, the ultimate goal being “to test, evaluate, and build these next-generation services.”
Justin Herman, the program’s head, told CoinDesk the effort was formed because new technologies, including blockchain and artificial intelligence, change more quickly than organizations can keep up with.
In an email, he said:
“Having a resource in the form of this Atlas is critical for federal agencies and the American people to identify opportunities to work together and avoid costly and time consuming pitfalls.”
Herman previously told CoinDesk that he wanted the ECT program to close the divide between the government’s interest in blockchain technology and its applications and knowledge that companies working with the tech already have.
As such, the program will update its Atlas every week, adding use cases, research updates and information on current projects being studied. The Atlas will also include resources “that anyone can use for evaluation, testing, and potential adoption,” according to the website.
Herman concluded: “This is only the beginning of the process to map out all of the critical work in testing, piloting and advancing our emerging technologies.”
CDP Clinic in Sisseton, South Dakota. Credit: cdphealth.com
That rural hospitals are struggling isn’t exactly a secret. More than 80 rural facilities have closed since 2010, and recent research from iVantage Health Analytics found that 41 percent of them are operating at a negative margin. Some of these hospitals are surviving by partnering with larger regional health systems. Some are changing their care delivery models entirely.
But others have found success simply by overhauling their electronic health records.
The functionality of many EMR systems is patchwork in nature, making it cumbersome for small staffs to handle things like billing and meeting meaningful use requirements. Fewer workers tackle more complex tasks, which makes it a struggle to operate in the black.
Make the EMR system simplified and more automated, however, and now these rural hospitals have got a fighting chance.
That’s been the experience at Rawlins County Health Center in Atwood, Kansas. Sharon Cox, Rawlins’ CEO,, and Destiny Schroeder, its information systems director, decided a more automated approach would help improve the hospital’s financial outlook, and so far, they’ve been right.
“We were running a couple of different systems that weren’t integrated, and this was an opportunity to do that,” said Cox. “One of the things you have to do in a hospital that’s small and with very few resources is you have to use technology to leverage resources, because we don’t have the staff or the expertise.”
There are different ways to streamline and automate an EHR system. Since wallets were light, Rawlins partnered with athenahealth to make the required overhaul. The turnaround was pretty dramatic, and put into stark contrast some of the deficiencies of Rawlin’s old legacy system.
“A big part of that was meaningful use and being able to meet meaningful use requirements,” said Schroeder. “That changes year to year, it seems, are there are more requirements that need to be done for that. With the legacy system we had, not all of our meaningful use data could be collected within one system. We had several different systems we had to go through that was kind of piecemeal … even to do day-to-day tasks. We’ve seen a huge difference with that. That’s made it a much easier process.”
“Small and rural hospitals see this as a foundational element to success in the future,” said Cox. “So many of those hospitals were looking at such dire circumstances, and how they were going to survive in the future.”
Workflow relief
One of the big things this has accomplished has been to take administrative tasks off providers’ plates — something that becomes especially important when staffing and resources are limited.
Rawlins has seen a huge change in its workflow — take charge entry, for example. Before the switch, the staff had to wait until the day-end close to enter those charges, and so they wouldn’t be seen in the account until the next day. Now, for the people in medical records, they can see all of the changes and see where they have results. That makes for a quicker workflow process; they can close the visit and drop a claim, whereas before it might have been strung out over several days.
Coteau des Prairies, a 25-bed acute care community hospital in South Dakota, has turned its financial picture around following a similar approach. For CEO Michael Coyle, the desire to streamline EHR stemmed in part from a lack of technical expertise on the part of the hospital’s small staff.
“We don’t have gurus here — we’re too rural,” said Coyle. “Whenever something went down, it seemed to take forever to fix. We’re a very busy hospital. The longer we’re down, the longer it takes to catch up. Burnout happens.”
A streamlined, automated EHR has helped staff avoid that burnout, and has made operations at the hospital much more efficient. That’s been reflected in Coteau des Prairies’ bottom line, which has improved substantially. That’s no small feat: The hospital has a high Medicaid population and sits close to a Native American reservation, with 60 percent of the overall population comprised of Native Americans.
“We meet with our client representatives every Friday and we go through what we need to be profitable,” said Coyle. “We’ve seen huge financial changes, probably upwards of seven figures. It will be close to a seven-figure turnaround by the end of the year. We’re doing front-end collections better than we ever have before. We’re not missing charges like we were in the past. And when the patient’s ready to go, the chart’s done, so you can print out a summary and take everything with you.”
Coyle said automated EHR systems are a requirement for survival in the rural healthcare market these days, at least for those facilities who are resistant to partnering with a larger health system. Further necessitating this shift is a rapidly changing healthcare system marked by uncertainty in Washington in regards to reform and how care is delivered — and paid for — in the future.
“Anytime you put the federal government into healthcare, it makes it more complicated,” said Coyle. “Just the little things, like the 340B program going away. That’s a huge revenue source for us. That’s how we pay for a lot of our charity care. And you’ve got to incentivize your providers. If they have to create a chart and they’re not creating (relative value units), they’re not making money. With all the changes that are coming, the technology we use needs to be functional, and it needs to respond to what the government is asking us to do.”
The numbers don’t lie. Since implementing the approach, Coteau des Prairies has seen a 20 percent reduction in cost, and a 20 percent increase in revenue — a 40 percent swing overall.
In two studies published today, one in Nature and another in Science, researchers from the Broad Institute of MIT and Harvard describe a new way to edit DNA and RNA, called base editing. The approach could one day treat a range of inherited diseases, some of which currently have no treatment options.
The human genome contains six billion DNA letters, or chemical bases known as A, C, G and T. These letters pair off—A with T and C with G—to form DNA’s double helix. Base editing, which uses a modified version of CRISPR, is able to change a single one of these letters at a time without making breaks to DNA’s structure.
That’s useful because sometimes just one base pair in a long strand of DNA gets swapped, deleted, or inserted—a phenomenon called a point mutation. Point mutations make up 32,000 of the 50,000 changes in the human genome known to be associated with diseases.
In the Nature study, researchers led by David Liu, a Harvard chemistry professor and member of the Broad Institute, were able to change an A into a G. Such a change would address about half the 32,000 known point mutations that cause disease.
To do it, they modified CRISPR so that it would target just a single base. The editing tool was able to rearrange the atoms in an A so that it instead resembled a G, tricking cells into fixing the other DNA strand to complete the switch. As a result, an A-T base pair became a G-C one. The technique essentially rewrites errors in the genetic code instead of cutting and replacing whole chunks of DNA.
“Standard genome-editing methods, including the use of CRISPR-Cas9, make double-stranded breaks in DNA, which is especially useful when the goal is to insert or delete DNA bases,” Liu said on a conference call with journalists on Tuesday. “But when the goal is to simply fix a point mutation, base editing offers a more efficient and cleaner solution.”
Liu said base editing isn’t meant to be a replacement to traditional gene editing with CRISPR, but rather another option for altering the genome in an attempt to correct disease. If CRISPR is akin to a pair of scissors, base editing is more like a pencil, he said.
Learn more about the original functionality of CRISPR, which scientists have now modified for improved precision.
Previously, researchers had created base editors capable of making the opposite kind of swap—changing a G into an A. Substitutions of a G for an A in certain parts of the DNA represent about 15 percent of disease-associated point mutations. In September, Chinese researchers reported that they used one of these editing tools in an embryo to remove the genetic mutation that causes anemia.
Working in cells taken from patients, Liu and his colleagues used their base-editing tool to correct a point mutation that causes hereditary hemochromatosis, a disorder that causes the body to absorb too much iron from food. This excess iron can build up over time and cause liver cancer and other liver diseases, diabetes, heart disease, or joint disease.
Liu and his team also used the base editor in human cells to induce a mutation that suppresses sickle-cell anemia. In both studies, they detected virtually no off-target effects, or unwanted DNA insertions or deletions, which are a concern with the traditional way of using CRISPR to edit entire genes.
In the new Science study, Feng Zhang, of the Broad Institute and MIT, used a similar base-editing method to target individual letters in RNA, DNA’s chemical cousin. RNA naturally degrades in the body, so editing RNA wouldn’t result in a permanent change to a person’s genome.
Ross Wilson, of the Innovative Genomics Institute at the University of California, Berkeley, says base editing may eventually be a better way to treat some diseases. He says a single base pair is like a word in a paragraph of text. With conventional CRISPR technology, you would have to replace the whole paragraph.
“It’s a lot of DNA to move around,” he says. With base editing, you could just change the single word.
Liu says he’s hopeful that base editing of DNA and RNA could be used as complimentary approaches for a “broad set of potential therapeutic applications.”
His lab is exploring base editing to fix blood disorders, neurological disorders, hereditary deafness, and hereditary blindness.
Dan Munro , ContributorI write about the intersection of healthcare innovation and policy. Opinions expressed by Forbes Contributors are their own.
I’m reminded of the character Vizzini (played brilliantly by Wallace Shawn) in the movie The Princess Bride – who keeps using the word inconceivable. Finally the character Inigo Montoya (played with equal brilliance by Mandy Patinkin) says:
“You keep using that word. I do not think it means what you think it means.”
It’s definitely conceivable that we’re seeing something similar with the use of the word disruption in healthcare. It’s embedded in the title of several books (by noted authors) and countless headlines through the years (now including this one). But like the character of Inigo Montoya – I’ve come to believe the word doesn’t mean what we think it means – for 3 really big reasons.
Training
Healthcare is one of the most expensive industries ever devised. By far the largest and most expensive portion of this industry (in terms of actual delivery) is services. The motivation, of course, has largely been born out of compassion to reduce pain and suffering – but let’s not kid ourselves either. Often the motives are simply big bucks greed. Here in the U.S., the greed part is fueled by a very simple free market equation: Demand (by patients) will always outstrip supply (of doctors). Always.
It takes about 10 years to train a doc. At graduation, the average medical student debt is about $160,000 (sometimes a lot higher). If you’re one of those fortunate graduates – you’re looking at how to pay back what amounts to a home mortgage – in the fastest time possible. Here are your options based on the average annual compensation by specialty.
Demand Distribution
Much of the interest, focus and attention around disrupting healthcare today continues to be on the low-acuity, primary and preventative sides of the system. That’s logical because it’s often at the entrance of the healthcare system and if you can’t (or won’t) change the supply chain – maybe you can have an impact on the demand side.
The problem is – that’s not where the big healthcare expenses are – and it doesn’t fundamentally change the system. We’ve also lost a fair amount of time (through the years) chasing the wrong bad guys – the insurance companies – which we conveniently blamed for much of the medical gluttony for the entire industry. Just like low-acuity healthcare – that’s not where the big dollars are being spent (and it’s certainly not where the big net profits are). Here’s the category breakdown of our National Healthcare Expenditure for 2010 (CMS data as published by the California Healthcare Foundation in 2012):
The net cost of health insurance is 6%. Nothing to sneeze at to be sure, but if you’re trying to “disrupt” a system that’s running at $3.5T per year (about 18% of GDP) is that really the best place to start? Just asking.
Startups Aren’t A Good Source For Disruption
Last month, Francisco Dao wrote a brilliant piece he called: “Why Startups Rarely Change the World” (here). What he said applies with equal strength to every sector – but perhaps more so to one that is almost entirely based on really (really) expensive services – healthcare.
… changing the world almost always requires massive amounts of money, groundbreaking technology, and a lot of time — three things most startups don’t have.”
Really big paradigm shifting developments are so costly and require such a long term outlook that they essentially have to be disconnected from the profit requirement*. As such, the only people who can afford to do this kind of work are the research labs of big companies (think Bell Labs in the old days and GoogleGOOG +0.43%
For those of you sharpening your anti-government pitchforks, where do you think the Internet came from? The government funded this experiment for decades without any expectation of profit and gave it to private industry for the rest of us to make money with. Everything we’ve done since then, from Amazon to underwear delivery, stands on the shoulders of profitless government funded research. Creating the Internet was the fundamental development that changed the world, not mailing crap in a box.
[* bold emphasis added]
That’s not to say there won’t be spectacular successes – with big valuations, big exits and windfall profits – but the real question remains. Are they truly disruptive at the core – or just around the edges?
Contrary to many who say our healthcare system is broken – it really isn’t. It is performing as it was designed. The people in it aren’t to blame – and we can absolutely change it – but we have to really want that change. That kind of change is at the core of the system –
with different goals, objectives and outcomes in mind. That’s much less of a technology problem and much more of process improvement one. Technology can – and will help – but all too often it’s a tactical overlay to try and patch the flawed system we’re living with today.
Unfortunately, this kind of change (dare I say disruption?) isn’t one that startups can deliver – and nor should we expect it from them. Just like startups, however, the kind of change we desperately need also has a big source of available capital. It just has a different street address. It’s not Sand Hill Road – it’s K Street. In terms of any attempt at comparison – it’s the difference between grind play on the slot machine (where many can and regularly do hit million dollar jackpots) and the private rooms of Baccarat for the whales that are flown in from around the world on private jets. As long as the whales are having fun – the casino (and slot machines) will remain open. Any way you look at that – it’s not disruption.
More than one in four Americans report difficulties paying for the prescription drugs they need
Understanding what drives pharmaceutical prices & spending will help policymakers develop effective policy solutions
Prescription drugs accounted for 17 percent of total U.S. health care spending — or about $457 billion — in 2015. And that share is expected to rise over the next decade as drug costs outpace those of all other health care services. Escalating drug costs have had a significant impact on consumers’ wallets. More than one in four Americans now report difficulties paying for the drugs they need.
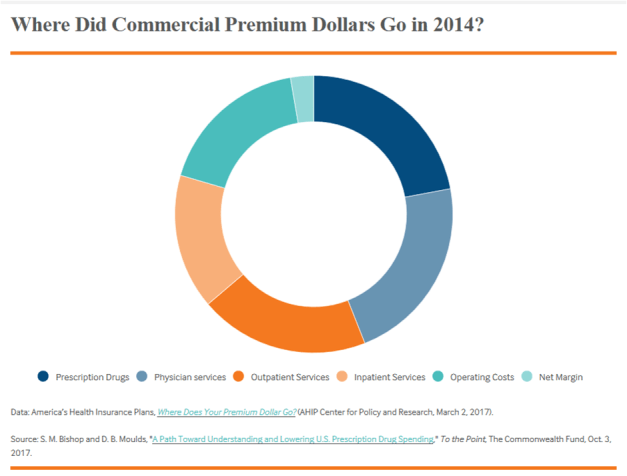
For individuals who purchase health insurance, or who have group coverage from their employer, prescription drugs account for the largest share of their total premium expense — 22.1 percent on average, according to the health insurance industry.
Prescription drugs are often by far the largest out-of-pocket health expenditure for people who rely on them for daily treatment, especially for those with chronic conditions such as rheumatoid arthritis, multiple sclerosis, or cancer. An increasing number of pharmaceutical interventions target small numbers of these patients at very high costs. Many such therapeutics carry price tags above $100,000 annually.
The skyrocketing cost of drugs has prompted a number of policy proposals at both the state and federal level. Many proposals aim either to bring down the amount we pay for drugs or to insulate consumers from their actual costs. Some proposed solutions are new: Maryland adopted an anti-price-gouging law for generics for which there is one manufacturer, while voters in California rejected a ballot measure that would have pegged the price paid for pharmaceuticals to the one paid by the U.S. Department of Veterans Affairs. Others are not so new: importing drugs from abroad has resurfaced as a potential tool for combating the high prices for drugs with little U.S. competition, and state legislators and members of Congress have introduced bills requiring payors to pick up more of their cost.
Reasons for high prescription drug prices are complex, and so are the potential policy solutions. Recently, The Commonwealth Fund launched a pharmaceutical spending initiative to support research and analysis that informs efforts to lower growth in overall spending on prescription drugs and make drugs more affordable to consumers. One project cosponsored with Memorial Sloan Kettering’s Drug Pricing Lab is producing 12 short “explainers” of fundamental but complex aspects of U.S. drug pricing published in Health Affairs from July through September. They will later be accompanied by several articles providing options for specific problems that have led to higher prices.
Another project, jointly funded with the Laura and John Arnold Foundation, culminated in a report by former Congressman Henry Waxman describing the root causes of high U.S. drug prices. Together with Senator Orin Hatch, Waxman authored the last major reform of U.S. pharmaceutical law — the Hatch-Waxman Act — which in 1984 extended patent protection for branded drugs and created a viable market for generic drugs. Congressman Waxman’s report takes the additional step of putting forth a framework for more reasonable drug costs. Waxman argues that prescription drug prices over the past decade reflect a distortion of the original balance Congress intended between pharmaceutical innovation and price competition. He proposes three goals: rebalancing incentives for innovation and pathways for price competition, so that manufacturers and patients both benefit from pharmaceutical market laws and regulations; prioritizing patient access and affordability; and better utilizing the available information on clinical value, comparative effectiveness, and pricing.
Both projects reflect a basic premise of our initiative: that the U.S. pharmaceutical market is far too expensive and opaque, and that making it less so is a critical first step in developing better policy to combat rising costs. Policymakers need unbiased information and insight into what drives pharmaceutical prices and spending so they can develop feasible, effective policy solutions. We intend to invest in research and analysis that will help policymakers realize this goal.
The October Kaiser Health Tracking Poll focuses on the Affordable Care Act’s (ACA) marketplaces as the November 1st open enrollment period approaches, amidst a period of uncertainty on the future of the individual market. The majority of the public think it is more important for President Trump and Congress to work on legislation to stabilize the marketplaces rather than continue efforts to repeal and replace the 2010 health care law (66 percent vs. 29 percent). There are distinct differences by party with the majority of Democrats (85 percent) and independents (67 percent) saying legislation to stabilize the marketplaces is more important while about half of Republicans (51 percent) say it is more important for lawmakers to continue efforts to repeal and replace the 2010 health care law.
One proposed step Congress could take to stabilize the markets and control costs for people who purchase their plans on their own is to guarantee payments to insurance companies that help cover the cost of deductibles and copayments for lower-income Americans (known commonly as ‘cost-sharing reduction’ (CSR) payments). The Trump Administration has announced they will stop making these payments. While initially the majority of Republicans (55 percent) say these payments should be stopped, when asked whether they support Congress guaranteeing the funds to continue the CSR payments when the proposal is included in a bipartisan compromise that would give states more flexibility in the types of plan sold in their state’s marketplace, a majority of the public (69 percent) – including roughly equal shares of Democrats (69 percent), independents (70 percent), and Republicans (68 percent) – support such a compromise.
Overall favorability of the ACA increased over the past month with about half (51 percent) of the public holding favorable views of the ACA while 40 percent hold an unfavorable view of the 2010 law. This is five percentage points higher than the share of the public who held favorable attitudes last month (46 percent), and more similar to the share measured in August.
Politics and the ACA Marketplaces
This month’s Kaiser Health Tracking Poll, which was conducted prior to President Trump’s executive order on the Affordable Care Act and the most recent statements from the Trump administration regarding CSR payments, examines the public’s attitudes towards the ACA marketplaces, before the next open enrollment period beginning on November 1st.
The majority of the public think it is more important for President Trump and Congress to work on legislation to stabilize the marketplaces in order to minimize premiums increases and encourage more insurers to participate in the marketplaces than continue efforts to repeal and replace the 2010 health care law (66 percent vs. 29 percent). There are distinct differences by party with the majority of Democrats (85 percent) and independents (67 percent) saying legislation to stabilize the marketplaces is more important while about half of Republicans (51 percent) say it is more important for lawmakers to continue efforts to repeal and replace the 2010 health care law.



 Oct 27, 2017 at 13:00 UTC by
Oct 27, 2017 at 13:00 UTC by 

 CDP Clinic in Sisseton, South Dakota. Credit:
CDP Clinic in Sisseton, South Dakota. Credit:  In two studies published today,
In two studies published today,