Numerous stakeholders have repeatedly called for improved health IT interoperability as a first step to improved healthcare but the Government Accountability Office (GAO) just released a report identifying ongoing barriers.
GAO reviewed 18 nonfederal initiatives geared toward advancing interoperability for the report. It did not reveal the initiatives included.
“Representatives from 10 of the initiatives noted that efforts to meet the programs’ requirements divert resources and attention from other efforts to enable interoperability,” according to the report. Representatives from 10 of the initiatives also called the Office of the National Coordinator for Health IT’s certification efforts insufficient to achieve interoperability.
The report identified two main issues hindering interoperability, according to those interviewed: the lack of incentives for providers to share data and Meaningful Use (MU) requirements.
The GAO report outlined the following other five other challenges to EHR interoperability:
Insufficient health data standards
Differing privacy rules across state lines
Matching patients with their health records
Costs associated with interoperability
Lack of agreements between providers to share health data
GAO selected the initiatives “judgmentally” and did not include all the approaches, challenges or actions related to achieving EHR interoperability so the information could not be generalized.
Seven of the 18 are focused on the creation of technical solutions such as “guidance to facilitate uniform implementation of standards” and five aim to encourage “providers or insurers to adopt certain policies and criteria.” The other six initiatives connect EHR systems through a technical service, enabling information exchange.
It is only after a revolution concludes that one can clearly look back and fully understand what triggered the revolution. External factors such as technology shifts can create the conditions for a revolution where it may not have been possible before. A generation that has a different worldview than their elders may not accept that status quo. From what I’m observing, I believe we are seeing a revolution’s first phase happen before our eyes.
I’m convinced that the only way there will be a true revolution in healthcare is if there is a partnership between clinicians and individual citizens (aka patients/consumers/people). One without the other isn’t sufficient to unseat deeply entrenched systems. However, I feel doctors will play a unique role in catalyzing the revolution (not to say that clinicians of all types won’t play important roles as well). As I’ve been a Johnny Appleseed of sorts chronicling the far-reaching and transformational work of doc-entrepreneurs, it feeds my optimism that it’s possible to overcome the “Preservatives” who have 3 trillion reasons to protect the status quo.
For those of us who have seen how much better the system can work when goals are properly aligned, it’s “good news” that doctor burnout and dissatisfaction is at an all-time high (see The Quadruple Aim: A Square Deal for Clinicians for more). Why? Dissatisfaction is the seed corn for change and revolution. Make no mistake. There is extremely high level of dissatisfaction amongst a large chunk of doctors who yearn for change. The contrast between those inside of flawed versus optimized care delivery and payment models is stark. One the one hand, I have heard and seen docs who are seeing 30-50 patients a day, dealing with unwieldy/outdated EHRs optimized for billing (vs. care) and getting more bureaucracy thrown on top of an already-flawed model. On the other hand, it’s breathtaking when I visit clinics like CareMore, ChenMed, Iora Health, Qliance, Vera Whole Health and others where the clinicians and patients are both extremely satisfied.
In the video below, Dr. Zubin Damania powerfully captures the sorts of internal dialogue doctors have had one by one with themselves.
When people would talk about their careers or their lives, the ones that were most passionate and were loving what they did always aroused in me an unease. It was almost an anger or jealousy and I would see them and go, “Why is he so happy and fulfilled and doing what he loves to do and I’m doing everything I’m supposed to do but I feel empty?” On the other side of this waking up and being who I am suddenly, I felt like, “Oh my god, that’s me now.”
I suspect all the doctor entrepreneurs/leaders I’ve highlighted below had some similar internal discussions. This is how revolutions begin. By no means is it limited to young doctors but typically it’s the young who foment revolutions and they are then joined by those older than them. As you can see in the picture accompanying this article after the post-Velvet Revolution celebration, it’s all ages who celebrate. It’s worth noting that the Velvet Revolution was triggered by a crackdown on students.
Ignoring Exponential Growth Has Devastating Consequences for Incumbents
Skeptics may say that these revolutionary practice models are a drop in the bucket and in most places, it’s business as usual. That is true just as it was true that the newspaper business looked fantastic in the late 1990s and early 2000s while digital media was going from tiny to small. However, the mistakes made by newspapers and their Zero Sum Game thinking were happening simultaneous to startups getting funding that would ultimately crush the most profitable portions of the newspaper business, not to mention create new sectors far bigger than the newspaper industry. Sadly (for the newspapers), they could have owned, invested or partnered with these players yet most arrogantly dismissed them.
Those startups were easy to ignore or diminish just as incumbent providers are blind to the exponential growth and funding (figures in parentheses) that organizations such as Aledade ($34.5M), Alignment Healthcare ($125M), Iora Health ($48.3M) and One Medical ($116.5M) are receiving. Further, other revolutionary organizations have already been acquired. CareMore was acquired for $800M by WellPoint and and HealthCare Partners was acquired for $4.4B by DaVita. It’s worth noting that the acquisitions weren’t by traditional providers. Rather, it was deep-pocketed players seeing an easy mark in soft oligopolistic health systems.
Change Starts at Home
Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has. – Margaret Mead
I put my family where my mouth is and convinced my folks to move into one of these revolutionary practices. They had been going to a well-regarded, large multi-specialty group in Seattle. However, the care they got was typical of our misaligned healthcare system. When my father was diagnosed with a significant chronic condition, he received a couple prescriptions from a specialist and told to check back in 6 months with the doctor. His PCP had no idea he’d been diagnosed with a significant condition. Meanwhile, his world came crashing down and a huge amount of anxiety and stress was thrust on him — surely, not the best “prescription” for his condition.
While it’s rarely easy to get someone to change their doctor, let alone a senior who has a significant condition, I ultimately prevailed in convincing my parents to make the move. Six months into being in Iora Health’s Medicare Advantage program, the change is dramatic. So much so that my dad told me last weekend he’d be happy to be a testimonial for them.
Creating the New Ecosystem
You never change things by fighting the existing reality. To change something, build a new model that makes the existing model obsolete. Buckminster Fuller
In their own way, each of the doctors listed below is contributing to building the new ecosystem and ignoring the Preservatives who are wedded to the status quo. As mentioned above, there are non-physician clinicians and individual citizens having a big impact but I focus on doc-entrepreneurs and intrapreneurs here.
Dr. Rajaie Batniji co-founded Collective Health in the belief they could help employees receive better care and coverage than what many experience with incumbent health plans
Dr. Steven Eisenberg for adding love & music to #oncology and humanity to medicine (h/t Bunny Ellerin)
The late Dr. Tom Ferguson coined the term e-patient many years before others were focused on equipped, enabled, empowered and engaged patients. This is a whitepaper (PDF) finished by his colleagues after his untimely passing.
Dr. Rushika Fernandopulle founded Iora Health to restore humanity to healthcare. They have proven to take on the most challenging patient populations and achieve outstanding outcomes and even take on individuals not addressed by the new health law with the support of a Nobel Prize winner.
Dr. Paul Grundy has led IBM’s transformation in healthcare shifting their thinking from healthcare as a soft benefits item left to HR to something that is a critical supply chain cost and source of competitive advantage.
Dr. Risa Lavizzo-Mourey is leading the Robert Wood Johnson Foundation spearheading their major re-focus on creating a Culture of Health that is impacting communities throughout the country.
Dr. Harry Leider is leading Walgreens retail clinic and telehealth expansionthat promises to reach half of the country by the end of the year.
Dr. Geraldine McGinty for her work creating innovative radiology payment models & spearheading payment reform (h/t Bunny Ellerin)
Dr. Farzad Mostashari described Aledade’s goals as follows: ”It’s to help independent primary care doctors re-design their practices, and re-magine their future. It’s to put primary care back in control of health care, with 21st century data analytics and technology tools. It’s to support them with people who will stand beside them, with no interests other than theirs in mind.”
Dr. Stan Schwartz saw what Dr. Keith Smith was doing and has been creating a true transparent medical network and making that available to employers — both doctors and patients are saved from excruciating amounts of bureaucracy in a very appealing economic model to both parties. It’s also the first Health Rosetta item to be delineated.
Four years ago, I observed how doctors such as Wendy Sue Swanson, Natasha Burgert & Howard Luks were doing something similar to how Sal Khan had “flipped the classroom”. This led to the Robert Wood Johnson Foundation initiating a major program called Flip the Clinic to improve outcomes and participation by patients.
Dr. Eric Topol has written and spoken extensively about how central the patient will be as a participant in their care compared to traditional practices. He highlights how the smartphone is the equivalent of the Gutenberg Press for medicine
Dr. Bryan Vartabedian is showing other doctors how to be a “public” physician & the impact that can have on outcomes
By no means is the list above complete. Add your comment below on a revolutionary doctor that has inspired you. Let us know what they are doing. Whether it is private practice, venture-backed startups, public health or health benefits, each doctor is contributing to the revolution. In their own way, they are fostering a Velvet Medical Revolution.
Dave Chase: Entrepreneur (2 exits), prof. speaker, new venture advisor, intrapreneur (2 $1B+ businesses), author & aspiring documentarian.
It was supposed to be a miracle, but now it’s what keeps Laura Bush, a nurse-practitioner near Albuquerque, awake at night.
There’s a drug called Sovaldi that works astonishingly well to cure people with the liver disease Hepatitis C. The rub? It costs $1,000 per day for all 12 weeks of treatment.
Bush’s clinic, First Choice Community Healthcare, is a federally qualified health center in the rural town of Los Lunas, New Mexico, which means she sees a disproportionate number of patients who are uninsured, underinsured, and on Medicaid, the government insurance program for the poor. In other words, they can’t afford Sovaldi.
The state’s Medicaid program rations access to Sovaldi and other blockbuster Hep C drugs to only the sickest patients. Even with those limitations, the drugs will likely cost the state an estimated $140 million this year. At various points since Sovaldi became available last year, Bush said, Medicaid has required her to perform risky liver biopsies on patients to prove how sick they are, or wait until patients have late-stage liver disease before they can be eligible for coverage. Each day, Bush juggles seeing patients with writing appeal letters and filing pre-authorizations that are often denied.
“Imagine if you went to get your mammogram, and they said, ‘you’ve got this [lump] here, but we’re not going to do anything about it until it gets bigger,’” Bush told me recently. “How would you take that, as a patient?”
With enough paperwork and tenacity, for a while Bush was able to secure free doses of Sovaldi directly from its manufacturer, Gilead Sciences. But that strategy, too, has become tougher in recent months after Gilead limited the types of patients who could receive free drugs.
New Mexico health-care workers aren’t the only ones struggling to secure these new treatments for their patients. Other states also require patients to be in late-stage liver disease, get urine drug screens, or prove abstinence from drugs and alcohol before they’ll consider covering them. Hep C patients commonly find themselves being forced to get sicker before they can get better.
Hep C is a liver disease transmitted by blood. It’s most common among baby boomers, most of whom contracted it through blood transfusions or by using contaminated needles to inject drugs. Left untreated, Hep C attacks the liver and can lead to cancer or liver failure.
Sovaldi costs $84,000 for a 12-week course of treatment, or about $1,000 per pill. It’s a great drug, working nearly 90 percent of the time and with few side effects. Sovaldi and the similarly pricey Harvoni, also made by Gilead, are a big improvement over older cures like interferon, which was only effective about half the time and whose side effects—rashes, fever, and nausea—were sometimes described as worse than the disease itself.
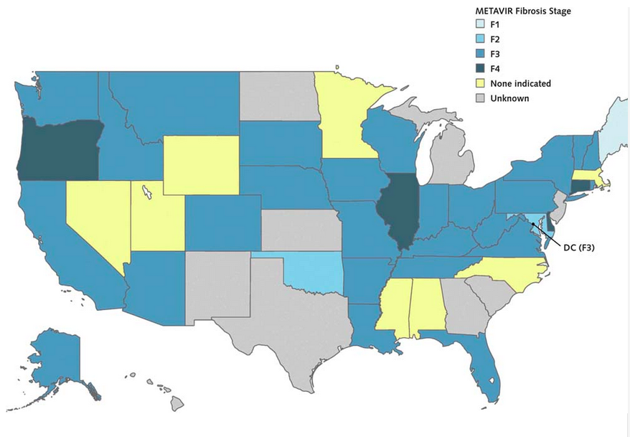
If state governments were to pay for Sovaldi or Harvoni for all of the Hep C patients on their Medicaid and prison rolls, the total bill would have been $55 billion. Most state Medicaid programs, therefore, are sharply limiting access to them. An August study in the Annals of Internal Medicine found that most states were only making these new drugs available to Medicaid patients who had advanced fibrosis, or liver scarring. Two-thirds required urine drug tests for drugs and alcohol before they would cover the medication. These measures, the study notes, are inconsistent with the recommendations of prominent health organizations and FDA guidelines.
Liver Disease Required for Medicaid Coverage of Sovaldi
State Medicaid programs, meanwhile, feel their hands are tied. “The states can’t afford it,” said Matt Salo, executive director of the National Association of State Medicaid Directors. “If we were to pony up for [Sovaldi], we would spend as much on this one drug as we would for all other drugs in the entire program. We don’t have the luxury of having a state legislature saying, ‘You want 5 to 10 percent more [money] this year? Cool, here’s your money.’ Many state legislatures are saying, ‘You’ve got to save, because revenues are down.’”
* * *
Martin Shkreli, the 32-year-old head of Turing Pharmaceuticals, stoked Internet outrage this week when it was reported that he raised the price of the 62-year-old anti-parasite drug Daraprim to $750 per tablet, from $13.50. Then he defended himself, Gekko-style, by saying, “I am a capitalist who plays to win.”
On Wednesday, he said he’ll lower the price to an undisclosed amount, but not before the parasite-free-organs-are-for-closers attitude drew widespread attention to the rising cost of prescription drugs. The prices of existing medications for everything from tuberculosis to blood pressure have rocketed up in recent years after the drugs were acquired by pharmaceutical companies.
“[Daraprim] is such a perfect, crystalline example of everything that can be done, given the lack of rationality in the system, and the total bankruptcy of the justifications for high drug prices in the first place,” Peter B. Bach, director of the center for health policy and outcomes at Memorial Sloan Kettering Cancer Center in New York, told the Washington Post.
But price hikes on existing drugs represent just a small part of America’s overall prescription-cost woes. Drug companies are regularly churning out new medications to treat everything from cholesterol to cancer. The $84,000 Sovaldi is practically nothing, for example, compared to Solirism, a $700,000-per-year drug that treats a rare blood disease, or Naglazyme, a $500,000 treatment for a rare skeletal disorder. The difference is that unlike drugs that only a few hundred Americans will ever need, Sovaldi could completely change the lives of the roughly three million Hep C sufferers in the U.S.
If, that is, their insurers would pay for it.
“I will at all costs try to get you the medication.”
Drug makers have long justified their high prices by saying it’s the only way they can recoup their investment into research and development. Then again, pharmaceutical companies have some of the largest profit margins in the health-care industry.
In an emailed statement, a Gilead spokeswoman responded to questions about Sovaldi’s price by saying, “unlike treatment for other chronic diseases, Sovaldi offers a cure … at a price that significantly reduces Hepatitis C treatment costs and delivers significant savings to the healthcare system over the long-term.”
Together, Sovaldi and Harvoni generated $12.4 billion in sales for Gilead last year. The company’s CEO, John C. Martin, is a billionaire. Gilead’s revenues doubled last year, and as the New York Times wrote, the company “now is faced with figuring out what to do with all the cash it is generating.”
* * *
Last year, New Mexico’s Human Services Department issued a rule that required patients to show that they have Stage 3 or Stage 4 liver fibrosis before Medicaid will cover them for drugs like Sovaldi.
In Stage 4, the liver is “hard as a rock,” Sanjeev Arora, a University of New Mexico physician, told the Albuquerque Journal. “Treating someone for Hepatitis C after they have developed cirrhosis is a little bit like closing the barn door after the horse has left.” While they wait to develop cirrhosis, Hep C patients face a higher risk of developing depression, nerve pain, and lymphoma.
When low-income Hep C patients come to see Bush, she’ll assure them that she wants to see them cured. “I will at all costs try to get you the medication,” she says.
If the person doesn’t have cirrhosis, she asks them to write a letter describing why they need Sovaldi. She’ll fill out a prior authorization and send it to Medicaid. If Medicaid denies the request, as she says often happens, she appeals. And on it goes.
Those who don’t get the medication can die “some of the worse deaths I’ve ever seen,” Bush said. People with end-stage liver disease vomit blood, feel confused, and turn yellow and bloated. “At the end you die not knowing who you are, your belly looks 12 months pregnant, you’re malnourished, and you’re bleeding to death,” she said.
Bush currently has about 20 patients waiting to get Sovaldi. One man doesn’t yet have cirrhosis, but he has trouble swallowing. His insurance won’t cover Sovaldi, which is a single-pill regimen, but will pay for a different treatment that requires taking multiple pills. Bush is worried he’ll choke.
Previously, Gilead sometimes provided free Sovaldi treatments to poor people who had been denied access to the drug by their insurer. But in July, the company changed its criteria and now only extends that offer to people who are uninsured. In the statement to The Atlantic, the Gilead spokeswoman said that the change was a response to insurers who were refusing to pay for Sovaldi. The assistance program “was designed to help uninsured patients with the most need, and changes are necessary to remain true to that mission,” she said.
Sovaldi’s story is not unique in America, but it is a uniquely American story. Other countries rigorously regulate the prices of prescription drugs, just as American cities set the rates of public utilities. In Germany, for example, the insurance-like “sickness funds” negotiate with both physician groups and drug manufacturers to determine the costs of all treatments. In the U.S., meanwhile, drug makers can simply name their price.
Sometimes, all of her attempts fail, and Bush has to tell her patients she can’t get one of these miracle pills for them. “I have one patient who got so upset because she thought I was blocking her ability to get the meds,” Bush said. “She came to me and said, ‘no one wants to give me the medications because I’m poor.’”
That woman finally did receive the drug, Bush said. It took seven months.
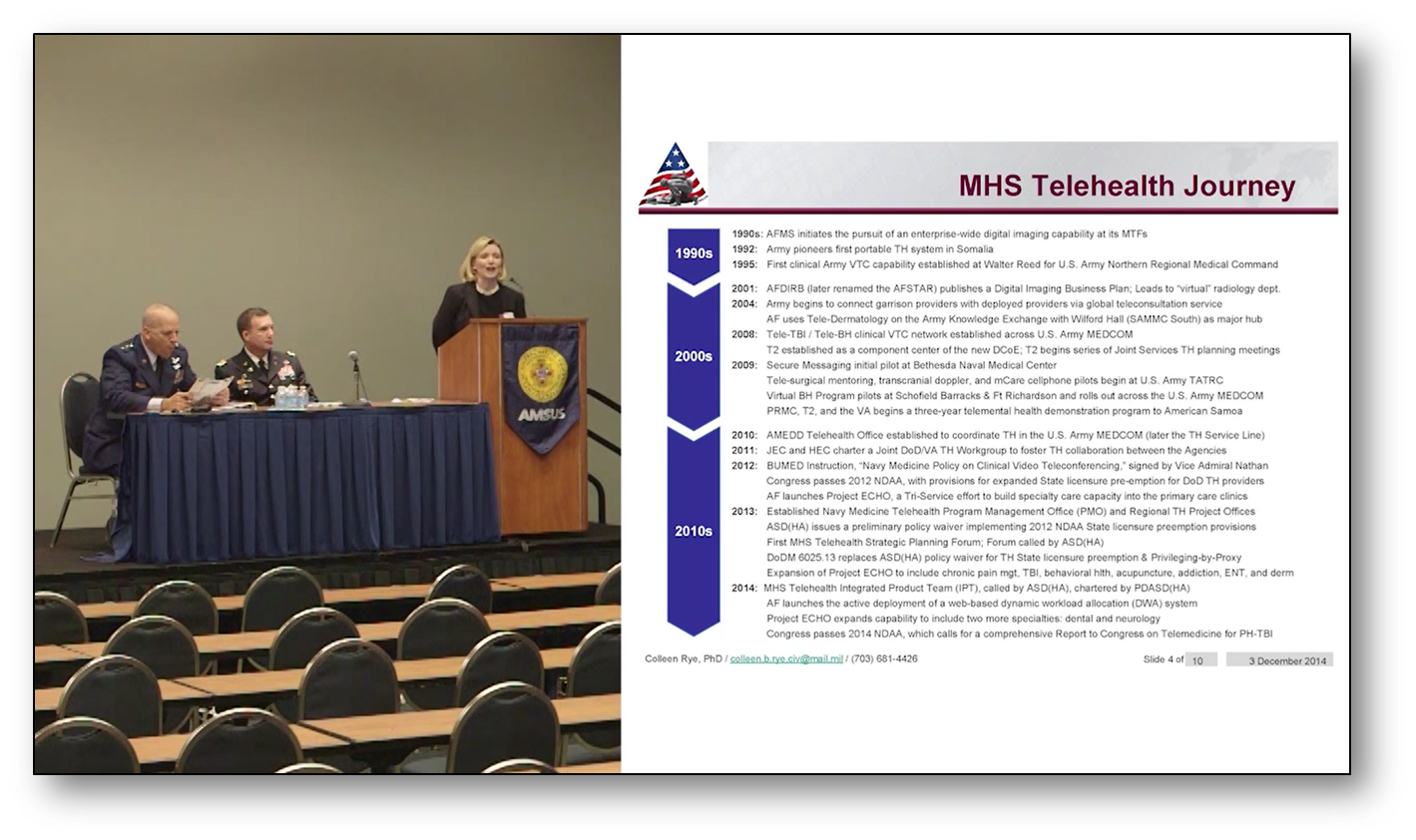
Dr. Jonathan Woodson, Assistant Secretary of Defense (Health Affairs), Plenary, Military Medicine: An Indispensable Instrument of National Security 2015 and Beyond, 3 December 2014
Dr. Carolyn Clancy, Interim Under Secretary for Health for the Department of Veterans Affairs, Plenary, Major Transition in VHA: The Blueprint for Excellence, 3 December 2014.
Friday 5 December 2014, Military Health System, Integrated Health Care System: Supporting a 21st Century Medically Ready/Ready Medical Force by MG Richard Thomas, MD and Ms. Mary Kaye Justis
Thursday 4 December 2014, Military Health System, Medical Modernization: Matching Requirements to Demand Signal by David Smith, MD, DASD Force Health Protection & Readiness
It’s no secret that EHR documentation has been a major pain point for physicians since the very beginning of the EHR Incentive Programs. Poorly designed software, a lack of familiarity with technology, the added burden of reporting for meaningful use and other quality initiatives, and a general sense that laptops are a significant obstacle in the patient-provider relationship have left a number of physicians apprehensive of using EHRs. Some physicians are so fed up with the EHR time suck that they have turned to medical scribes to do the heavy keyboard work instead.
While this initially seems like the perfect way to improve efficiency, not everyone is convinced that EHR documentation produced by these scribes – credentialed data entry experts who typically do not hold a medical license – will be a positive development for the EHR industry. A team of experts from CHRISTUS Health in Texas, led by George A. Gellert, MD, MPH, MPA, argue in a JAMA viewpoint article that scribes are just a temporary bandage for a much deeper wound: the inability of the EHR vendor community to produce software that allows physicians to do their own documentation without losing minutes or hours each day on data entry.
With the rise of data analytics pressuring the healthcare industry to produce consistently clean, complete, and accurate documentation, the focus on data governance has never been stronger. Medical scribes may not be allowed to create documentation independently of their supervising physician, according to The Joint Commission, and CMS may frown upon the notion of scribes being able to enter orders using CPOE systems, but they still create an added layer of interference between the physician and the chart, which may increase the potential for human error.
“With problems associated with EHRs so substantial—and physicians’ experiences using medical scribes so positive—are there any risks engendered by the rise of a medical scribe industry and its potential for becoming integral to US health care delivery?” Gellert asks. “Despite scribes’ reported value, this industry should be viewed as what it is: a workaround or adaptation to the suboptimal state of today’s EHRs.”
Gellert fears that the rise of medical scribes may lead EHR developers to push innovation off their lists of top priorities, leading the industry to “a deceleration and possibly stagnation in EHR technological improvement.” Relying on scribes to do the dirty work of EHR documentation may also lead physicians to relax their view of what their helpers should or should not do, and might even lead to scribes operating outside of their purview as the lines blur. After all of the progress the industry has made towards utilizing electronic data for quality initiatives and clinical analytics, will scribes push the healthcare ecosystem back into the ignoble mire of lackadaisical documentation and inadequate data governance?
Not according to physicians who use them. A 2013 study at the United Heart and Vascular Clinic in Minnesota found that medical scribes cut down patient consult prep time by one third and saved close to $2500 per patient in direct and indirect costs, says study author Dr. Alan J. Bank.
“To me, it doesn’t make economic sense to have a doctor who’s getting paid a good salary and has all the training to be sitting there typing or filling out forms,” Bank told EHRintelligence. “Someone else can do it just as well or better. And a lot of physicians are getting worn out. They’re just getting tired. But if we made things easier for physicians and took some of the paperwork away, it would be better for everybody. As doctors, we want to take care of patients. We don’t want to be typists.”
Medical scribes may indeed be a workaround for software that does not adequately meet a physician’s needs, but even Gellert admits that after years of EHR vendors competing for a white hot market of meaningful use hopefuls, the industry has not been able to conquer its data governance and health information management challenges. “Even after a decade of use, some EHRs and CPOE may not compete with the speed of a paper checklist, and may never,” he writes, but maintains that physician pressure on the commercial market, if applied consistently and firmly, will lead to heretofore unseen leaps in EHR innovation.
But while the industry is waiting for these improvements to be made, should they suffer with the potential for financial losses, the rampant dissatisfaction, and the risk of burnout that is reducing an already inadequate number of physicians operating in a rapidly changing industry? Or can medical scribes provide a useful stopgap and necessary support to physicians on the brink of calling it quits? Gellert believes that once a physician uses a scribe to relieve the pressure, it’s only a matter of time before that scribe becomes indispensable, despite the risks and perhaps despite the eventual availability of improved technology. The risk is simply too high to justify the short-term benefits, he says.
“The answer to today’s inadequate EHRs is not scribe support,” he concludes. “The use of scribes can pose potential risks to patients if they are allowed to enter orders into the EHR, and the risk of use creep is high. The medical scribe industry may impede the technological evolution of EHR products by undermining market demand for needed improvement, and it is unlikely that scribes will be used only as a temporary solution. The rise of the medical scribe industry should not be a substitute for much-needed EHR innovation and transition to more highly effective and more functionally efficient EHR systems.”
For people living in Wyoming or South Dakota or rural Virginia, a trip to the cardiologist isn’t a simple undertaking. “They’re taking a whole day off work to drive 150 miles, go the appointment, and drive 150 miles home,” says Deanna Larson, senior vice president at Avera Health. That’s why Avera, which runs a network of over a hundred clinics and hospitals in the upper midwest, has invested in telemedicine, allowing doctors to pop into rural clinics by video from hundreds of miles away.
Telemedicine has been a buzzword for years now, but the rural communities that could benefit most from it also have the least access to fast and reliable Internet—an obvious prerequisite. That’s not for lack of political effort. The Federal Communications Commission has been responsible for helping connect rural healthcare facilities since the Telecommunications Reform Act of 1996. The Internet has changed since then: Bulky desktops have shrunk to pocket iPhones and 56 kpbs dial ups have been superseded by 35 Mbps connections—nearly 10,000 times faster. The 20-year-old law, even after a few revisions, has struggled to keep up.
Telemedicine infrastructure is lagging on two fronts. First, many rural clinics have Internet access that is still too slow and unreliable. Second, telemedicine is increasingly moving from the clinic into the home, with at-home monitoring and mobile apps. Here, the facts on the ground are even worse: According to the FCC’s 2015 Broadband Progress Report, 55 million Americans still do not have access to broadband speed Internet access, which includes more than half of rural Americans.
The FCC’s rural health care program can give out $400 million every year to link up rural health facilities. “It’s never reached anywhere near that limit,” says Jonathan Linkous, CEO of the American Telemedicine Association. In 2013, the rural health care program paid out $159 million. Linkous chalks up it up the program’s complex bureaucracy, which the overworked staff members at rural clinics don’t have time to navigate.
Rural clinics do have usually have broadband connections now, but they can be T1 lines, which top out at just 1.544 Mbps. (In comparison, Comcast offers cable Internet up to 150 Mbps in the San Francisco area.) Avera requires its facilities to have a T1 line, and it lays lines for ones that do not, like for a facility in remote Montana. That’s fast enough for a video consult, but it’s not necessarily enough for, say, an electronic intensive care unit, in which healthcare professionals remotely monitor patients who need critical care. “There are significant rural areas that still do not have the speed necessary to do the telemedicine they would like,” says Alan Morgan, CEO of the National Rural Health Association.
Tap or Swipe for the Doctor
As broadbroad in rural health facilities is still lagging behind, mobile health apps are blowing the problem wide open. “If you’re still providing broadband to brick and mortar, you’re going to where healthcare used to be,” says Linkous. “More and more, you have to get beyond the traditional walls of hospitals and clinics.”
In 2014, for example, the University of Mississippi Medical Center began a pilot program that sent 85 patients with uncontrolled diabetes home with a tablet. The tablet kept track of blood glucose levels and sent real-time data back to a team of doctors. The first six months of the study have been promising: The diabetes patients lost weight and reported getting their diabetes under control.
But for programs like this diabetes pilot to work, patients need reliable Internet access at home. That’s not a given, with half of rural Americans still lacking broadband-level speeds. And if you’ve ever driven across the country, you’ve certainly driven through vast tracts of land without cell phone access. The FCC and the US Department of Agriculture both have programs dedicated to promoting rural broadband—modeled after the 20th century push for rural telephone service. But the programs haven’t been as widely successful yet. The USDA’s Rural Utilities Service, especially, has come under fire for spending money in all the wrong places.
One bright spot is the FCC’s recently proposed changes to its Lifeline program, says Linkous. Lifeline has given millions of low-income Americans a $9.25 per month subsidy to pay for a mobile or landline phone, and the FCC is now considering broadening the program to include broadband. WIRED readers, of all people, can probably get behind universal Internet access—but the FCC’s decision could actually help make that real.