Video: Health Systems of the Future (French) (HTML)
Video: Health Systems of the Future (Spanish) (HTML)
Poor-quality health care around the globe causes ongoing damage to human health. In low- and middle-income countries (LMICs), between 5.7 and 8.4 million deaths occur each year from poor quality of care, which means that quality defects cause 10 to 15 percent of the total deaths in these countries. The resulting costs of lost productivity alone amount to between $1.4 and $1.6 trillion each year.
A move toward universal health coverage (UHC) is the central theme of global health policy today, but the evidence is clear: Even if such a movement succeeds, billions of people will have access to care of such low quality that it will not help them—and indeed often will harm them. Without deliberate, comprehensive efforts to improve the quality of health care globally, UHC will be largely an empty vessel.
With support from 7 sponsors, the National Academies of Sciences, Engineering, and Medicine undertook a study to examine the global impacts of poor-quality health care and to recommend ways to improve quality while expanding UHC, particularly in low-resource areas. The resulting report, Crossing the Global Quality Chasm: Improving Health Care Worldwide, builds on the work of the landmark 2001 Institute of Medicine (IOM) report Crossing the Quality Chasm by calling attention to the gaps in health care quality that still remain globally and suggesting approaches to bridge them.
Kim Bellard Editor at Tincture. Always curious, always ready to challenge the status quo, in health care & elsewhere, especially via innovation & technology.
A few recent stories are, I believe, reaffirming one of the big problems about healthcare: hospitals are 19th century institutions operating under 20th century business models in the 21st century. It’s time to rethink what we want a “hospital” to be.
The Boston Globereported on Stanford’s new Lucile Packard Children’s Hospital, which cost a cool $1.3 billion and is touted as, of course, the “hospital of the future.” As they describe it, it doesn’t look like a hospital at all, but rather: “It is some hybrid of hotel, museum, and high-tech laboratory.”
The Globe notes a similarly ambitious, $1.2 billion renovation at Boston Children’s, along with big hospital projects in numerous other cities. “These hospitals are kind of high-tech hotels,” Mark Wietecha, president of the national Children’s Hospital Association told the Globe. “Everybody’s competing by building cooler hotels. They can do more, save more lives, all good stuff — but not cheap.”
Then there was the NBC News story on the debacle with the new VA hospital in Denver. Again, it’s big and beautiful, another “cool hotel.” However, it took 14 years to plan and build — 5 years late — and its costs ballooned from $328 million to, umm, $1.73 billion (and counting…), despite somehow neglecting to include a place to treat PTSD, which will require further investments.
Meanwhile, the VA continues to struggle with how to improve access to services for veterans generally.
The problem is that hospitals are big and getting bigger, going from building to buildings to campuses. They are expensive and getting more expensive. At some point, we have to ask: is this really how we want to spend our healthcare dollar?
Some hospitals are figuring other ways to spend their — I mean, “our” — money on our health. Take Nationwide Children’s Hospital. Located in a somewhat blighted neighborhood of Columbus (OH), its Healthy Neighborhoods Healthy Families (HNHF) program “treats the neighborhood as the patient,” as their summary in Pediatrics put it.
The hospital is leading a partnership that has built 58 affordable housing units, renovated 71 homes, given out 158 home improvement projects, and helped spur a 58 unit housing/office development. They’ve also hired 800 local residents and instituted a jobs training program.
They’re already seeing lower murder rates, higher high school graduation rates, and are studying impacts on emergency room visits, inpatient days, and rates of specific conditions such as asthma.
It’s essential if we want to change things. Every city has certain pockets of disadvantage. Those particular pockets account for a disproportionate share of all the challenges children face. . . if you’re a pediatrician and you look at the numbers, you have to do something to participate in the solution around eliminating poverty in these neighborhoods. Medical care’s never going to change some of these outcomes.
“This is a national trend,” Jason Corburn, professor of city and regional planning at the University of California, Berkeley, told NPR. “It’s happening in cities across the country,” citing similar efforts in Atlanta, Boston, New York, and Seattle.
Or take a program, led by researchers at the University of Pennsylvania, that focused on cleaning up vacant lots in Philadelphia. It sounds simple, but resulted in significant improvements in residents’ mental health. The authors concluded: “Making structural changes to the lowest-resource neighborhoods can make them healthier and may be an important mechanism to address persistent and entrenched socioeconomic health disparities.”
…there’s something that’s actually important about the green space…It’s a relatively low-cost intervention … and it’s a pretty simple intervention. It’s very simple to replicate. It’s not complicated and could be easy for a city that hasn’t done this.
Or a hospital.
It is true that hospitals (excuse me, “health systems”) are diversifying — building/buying satellite locations, free-standing emergency rooms, urgent care centers, and physician practices — but those big buildings remain the locus, and their sunk costs weigh on hospitals’ finances.
There’s a great quote from Philip Betbeze of HealthLeaders: “the future of the hospital is not a hospital.” The future requires, as Richard Darch, CEO of Archus, more recently wrote, “radically and fundamentally rethinking the hospital, and even discarding the term ‘hospital’ to the history books.” Mr. Darch sees hospitals as “anchor institutions” of their communities, with a greater focus on wellness and structured more as a campus than a single place.
I’d go further: not a building, not even a campus, but as a dispersed array of services — some medical, many not — that are delivered as close to our homes as possible (and, preferably, in our homes).
Do an image search for “hospital of the future” and you’ll get pictures of futuristic buildings with some cool-looking technologies thrown in. What I want to see are images of services being delivered where I am, focused around me, aimed at my convenience — not at the convenience of the people delivering my care.
Some will argue, well, we’re not going to do surgery at home. We’re not going to have NICUs at home. We’re not going to put doctors and nurses in every sick person’s home.
Perhaps, but there are a lot of things we’re now doing in hospitals that don’t need to be. There are a lot of expensive devices that are now centralized in hospitals that could be decentralized or even made mobile. There are a lot of interventions that aren’t medical at all.
It requires us blowing up our concept of a “hospital.”
Don’t donate money for hospital expansion/renovation plans. Don’t buy bonds for them either. Don’t sit passively on hospital boards that push for them or expensive new equipment.
Instead, we should be questioning: how can a “hospital” most impact our communities’ health? What kinds of investments in our communities’ health can they be making? How we do push healthcare and health down as close to where and how people live as possible?
The argument will always be, well, payors won’t pay for those kinds of things. The business models don’t support them. To that I say: it’s time not just for new kinds of “hospitals,” but also new kinds of business models.
Practitioners and policymakers have become increasingly aware in recent years that achieving good health and economic vitality in neighborhoods requires the close collaboration of a variety of sectors, including housing, education and social services. But collaboration does not occur in a vacuum; institutions often provide a crucial focus for collaboration and are active agents—or “hubs”—in the process.
In “Hospitals and schools as hubs for building healthy communities (PDF),” Stuart Butler and Carmen Diaz feature two such institutions that can play a major role in helping to enhance health and long-term economic mobility in a community: hospitals and schools. They have enormous potential as hubs, but also face obstacles and challenges associated with such things as data sharing, budget and payment issues, and inflexible business plans.
This report, produced with advice from an advisory group of researchers, policy experts, and practitioners in health and education, recommends policy steps and other actions that would create an improved environment in which hospitals and schools could play a much greater role as hubs in communities. These include:
Improving the collection, use, and sharing of data among sectors to facilitate partnerships.
Making greater use of intermediaries.
Widening the skill sets of school and hospital leaders and key staff.
Making use of the community obligations of nonprofit hospitals and financial institutions, as well as the community focus of the new education statute, to help launch creative, coordinated partnerships.
Making greater use of waivers, demonstrations, and other steps to foster hubs and other partnerships.
Taking steps to facilitate the braiding and blending of public and private resources from multiple sectors and sources.
Editor’s Note: This article originally appeared in Real Clear Markets on August 14, 2018.
It is no surprise that partisan gridlock in Washington triggers widespread concern about the future of our health system. It is not just that there are worries about the future cost and availability of coverage for families. It is also that Congress seems quite unable to settle on a permanent framework for 18 percent of the entire US economy.
Still, we should temper our anxiety about deep disagreement and legislative paralysis hampering the long-term management of this vital part of the economy. That’s because there are at least three reasons for some cautious optimism.
First, the genius of our system of federalism allows organizational design innovation to evolve in the regulation and public management of our health care sector despite intense disagreement at the national level. For instance, when there are national-level disputes about the best way to achieve stable insurance markets to cover high-cost people at reasonable premiums, or to care for the frail elderly, state-led federalism allows alternative strategies to be tried and compared and agreement to emerge. That is currently happening because federal law gives the federal government power to grant waivers to states to modify some programs within the state’s borders. For instance, the Trump Administration currently is granting federal waivers to permit some states to experiment with “high risk pools” that subsidize high cost individuals while lowering premiums for families with lower average health costs.
True, such experiments do not always succeed, and the waivers tend to reflect the perspective of each federal administration, as well as the political culture of the state requesting a waiver. So there have to be safeguards. But this experimentation, over time, can significantly improve the operation of the health system. Not only that, state leadership and experimentation can also help a national consensus to develop in areas where there had once been deep disagreement at the national level. We saw this in the 1990s in the case of welfare reform, and more recently in the state-led acceptance of gay marriage.
Second, there is a growing recognition that there is much more to achieving good health than just spending money on medical care. We could save billions of dollars repairing hip fractures for seniors, for instance, by investing a fraction of that money in such things as safer bathrooms and non-slip carpeting. Meanwhile, tackling stress and abuse affecting young children can sharply reduce downstream mental health costs.
The problem is that while other countries achieve better health results by improving the balance between medical and social service spending, America is the outlier by over-medicalizing health. But the good news is that all over the country, often with federal encouragement, there are more and more efforts to incorporate non-medical services to boost health outcomes. For instance, Vermont’s “SASH” program coordinates medical and social services to improve health outcomes for the elderly. Meanwhile federal waivers are allowing state Medicaid programs to use funds on housing and social services that improve health. And new federal legislation permits Medicare Advantage plans to use some funds for health-related transportation and other non-medical services.
These initiatives mean the health system is gradually changing, quietly, and in a bipartisan way, despite gridlock at the national level. Over time the resulting change could be profound.
And third, there is the wild card of “disruptive innovation.” We tend to think of health care innovation only as breakthrough drugs and surgeries, or perhaps organizational developments like the growth of local urgent care centers and telemedicine. But far more radical change can happen when huge new players enter an industry. Remember how Steve Jobs and Apple transformed the music industry, or how Amazon upended not only the selling of books but the selling of everything.
The health industry is ripe for a similar dramatic transformation from the outside. After all, except for new technology, the hospital and doctor’s office model has changed little in well over a hundred years. Powerful new entrants like the joint venture of Amazon, JPMorgan Chase and Berkshire Hathaway could be dramatic agents of change. There is a reason that people like Jeff Bezos and Warren Buffet are billionaires – they perceive opportunities for transformation that the rest of us don’t see. Whether this particular venture will be the Jobs-style gamechanger remains to be seen, but two things are clear. Transformative disruption is coming in health care. And federal legislation is generally irrelevant to this kind of radical industry restructuring.
These four patterns are going on to a large extent under the radar. They do not depend on bipartisanship and legislative breakthroughs in Washington. But they are altering the health industry in positive ways while we wait for Congress to get its act together.
However, becoming a doctor remains one of the most challenging career paths you can embark upon. It requires extensive (and expensive) schooling followed by intensive residencies before you’re fully on your feet. The idea, generally, is that all the hard work will pay off not only financially, but also in terms of job satisfaction and work-life balance; then there’s the immeasurable personal benefits of helping people, and possibly even saving lives. In terms of both nobility and prestige, few occupations rank as high.
So why is there waning interest in being a physician? A recent report from the Association of American Medical Colleges projected a shortage of 42,600 to 121,300 physicians by 2030, up from its 2017 projected shortage of 40,800 to 104,900 doctors.
There appear to be two main factors driving this anticipated doctor drought: First, young people are becoming less interested in pursuing medical careers with the rise of STEM jobs, a shift that Craig Fowler, regional VP of The Medicus Firm, a national physician search and consulting agency based in Dallas, has noticed.
“There are definitely fewer people going to [med school] and more going into careers like engineering,” Fowler told NBC News.
Fowler also speaks to the desire among millennials to be in hip, urban locations — a luxury you likely won’t get when you’re fresh out of medical school and in need of a residency.
“This is why places in middle America hire firms like ours,” Fowler said. “They’re having a harder time attracting people.”
But perhaps the more interesting story lies not with those deciding to eschew medical degrees; it’s with the people who went through all that training, who became doctors — and then decided to opt for another path.
This drastic career change can be a result of new med school grads being unable to find a residency within a reasonable period of time.
“Graduating med school doesn’t mean you’ll get into a residency,” said Fowler. “There aren’t enough residency slots for medical grads. So you have that population of people who have an MD but didn’t practice for that reason. There is this bottleneck effect.”
The mounting bureaucracy
This “bottleneck effect” doesn’t usually sour grads on staying the course, Fowler finds, but he does see plenty of doctors in the later stages of their careers hang up their stethoscopes earlier than expected. Some cite electronic health records (EHRs) as part of the reason — especially old school doctors who don’t pride themselves on their computer skills. New research by Stanford Medicine, conducted by The Harris Poll, found that 59 percent think EHRs “need a complete overhaul;” while 40 percent see “more challenges with EHRs than benefits.”
And then there are those doctors who left medicine because the cons of the job started to far outweigh the pros.
“After 20 years, I quit medicine and none of my colleagues were surprised. In fact, they all said they wish they could do the same,” Dr. Amy Baxter told NBC News.
“I began to feel like an easily replaceable cog in the health care machine. With the [enforcement] of EHRs, I had to spend more time as a scribe. One night a child I was treating had a seizure and I couldn’t get the medicine to enable them to breathe because their chart wasn’t in the system yet. This kid was fixing to die and I, the doctor, couldn’t get the medicine. It was demoralizing.”
Baxter left pediatric emergency medicine to head a company that develops physiological products for personal pain management.
Dr. Ha-Neul Seo, director of global recruitment at EF Education First in London, was a general practitioner in the U.K. for several years before heading to the U.S. to study health care management and policy. She wound up leaving medicine to focus on education because she felt, to some extent, she’d defaulted into a career that turned out to be more tedious than expected.
“As a patient you want your doctor to love and be passionate about their work — and I realized that wasn’t me,” Seo said. “Some parts were incredible, but the moments when I felt I was making a true difference were too few and far between. And then there was the issue of work-life balance. I had my first child and was barely seeing him. The schedule was relentless.”
Dr. Nicole Swiner, a physician and author, has stuck with being a doctor because she loves it so much, but she deeply empathizes with those who decide to leave.
“It has gotten worse for all of us, unfortunately — whether you work in the hospital or in the outpatient setting,” she told NBC News. “We are burdened more by nonmedical business or insurance professionals without any medical training. It’s disheartening. I have transitioned to more part-time clinical work [so as to focus more on] speaking, writing and consulting.”
“Become a full-time consultant, author, speaker, entrepreneur, baker, cheerleader — whatever. Just be happy. Life’s too short,” Swiner said.
by Jeff Coughlin, senior director, Federal & State Affairs, HIMSS
The Centers for Medicare & Medicaid Services (CMS) and Office of the National Coordinator for Health IT (ONC) have published several proposed rules, draft guidance documents, and requests for information (RFIs) – as well as one final rule – over the last several months. By and large, these measures have focused on supporting the shift to a value-based care delivery model, and away from a fee-for-service, volume-driven environment.
HIMSS continues to pay close attention to these government actions and is looking for opportunities to ensure that health information and technology are appropriately positioned in these efforts. Here is a roundup of some of my key takeaways thus far from these government actions.
It’s Not Business as Usual Anymore
The Trump Administration has spent its first 20 months in office re-evaluating every policy decision made during the Obama Administration and determining if there is a different approach they want to take. In addition to their work on the Affordable Care Act, President Trump’s Department of Health and Human Services (HHS) has undertaken extensive changes for other programs, such as the Meaningful Use Program (now Promoting Interoperability), Quality Payment Program (QPP), Medicare Shared Savings Program, quality reporting paradigms, and interoperability/data sharing initiatives. HHS is headed toward finalizing significant modifications of previous policies – for many of the reasons discussed below – and exhibiting a real openness to consider new directions.
Many changes have been legislatively driven (through enactment of the 21st Century Cures Act, for instance), but there has also been a real willingness to re-interpret existing statute. Thus far, changes that have been implemented on telehealth and remote patient monitoring in the 2018 Physician Fee Schedule (PFS) – with potentially more adjustments on the way in the 2019 QPP/PFS Proposed Rule – and, CMS is considering far-reaching changes to the Medicare/Medicaid Conditions of Participation as well as the Physician Self-Referral Rule. Evaluating changes in many of these areas is long overdue, but I think that it’s taken a fresh perspective from a new Administration to even ponder publication of these RFIs and to consider future modifications.
One cross-cutting theme has been a real focus on the patient – activating, engaging and prioritizing the needs of patients. A major part of this work is reliant on greater data exchange by breaking down the barriers that prevent patients from having electronic access and true control of their own health records from the device or application of their choice. This theme is being operationalized in several programs, including:
MyHealthEData Initiative: Empowers patients by giving them control of their healthcare data, and allowing it to follow them through their healthcare journey
Medicare’s Blue Button 2.0: Creates a new and secure way for Medicare beneficiaries to access and share their personal health data in a universal digital format, by enabling traditional Medicare beneficiaries to connect their claims data to the secure applications, providers, services and research programs they trust
The overarching focus that CMS and ONC are putting on the patient is impressive and will likely continue to be built upon in future actions.
Looking to Leverage Information and Technology
Most of the topics that I have raised are dependent upon information and technology – whether its data exchange, telehealth, the promise of electronic health records, or Blue Button 2.0, each plays an important part in supporting the shift to value as well as delivering even better and safer care. The portfolio of issues that we must address in health IT advocacy is ever-expanding given the growing importance of information and technology across the entire healthcare sector. CMS, ONC, and the entirety of agencies within HHS, are finding new and innovative ways to leverage health information and technology across their programs and increase its applicability in burgeoning areas.
Clinician Burden is Front and Center Across All Programs
The path that HHS is pursuing to implement all these programs is extremely cognizant of minimizing or reducing the burdens that are placed on clinicians, which the Department is referring to as the Patients Over Paperwork Initiative. CMS and ONC are looking at this issue holistically, and are including regulatory, administrative, documentation and reporting burdens in their review and action plans (HIMSS collaborated to submit comments on some potential solutions in June 2018).
The idea behind minimizing burden is very patient-focused – with relieving burden defined as an opportunity to spend more face-time with patients and eliminating the unnecessary actions that occur in the course of clinical practice.
CMS has already recommended great strides to reduce burden, especially in the 2019 PFS/QPP Proposed Rule, by streamlining Evaluation and Management documentation and payment processes as well as other changes on the QPP side.
Overall, CMS and ONC are using their burden-related actions to help practitioners deliver better care by allowing them to focus their time on actions that make sense and appropriately using information and technology.
So, What is HIMSS Doing?
The HIMSS team continues to build up our portfolio on all these issues, trying to understand the specifics and nuances so that we can not only advise the government, but inform our members on HIMSS’s perspective and help them magnify our advocacy messages across the community.
We want to continue to position HIMSS as a thought leader and advocate for supporting the shift to value-based care and how information and technology contribute to that future state, as well as more ubiquitous and seamless interoperability, greater innovation in the field, and better engagement and activation of patients.
We’re on the right path – and, we’ll keep working to ensure that we’re heard and at the forefront of any government policy actions.
If you have comments, further thoughts, or want to get involved in our advocacy activities, please feel free to reach out via email.
Upcoming Policy Webinar
Leveraging Health Information and Technology to Mitigate the Opioid Crisis: Policy Landscape and Steps Forward
Part 3 of 3: September 6 | Register
Part 2 of 3: Listen to webinar
Part 1 of 3: Listen to webinar
The path to value-based care in healthcare is becoming murky. After a few years of heightened promise and hope, the current and near-future reality is not necessarily so promising.
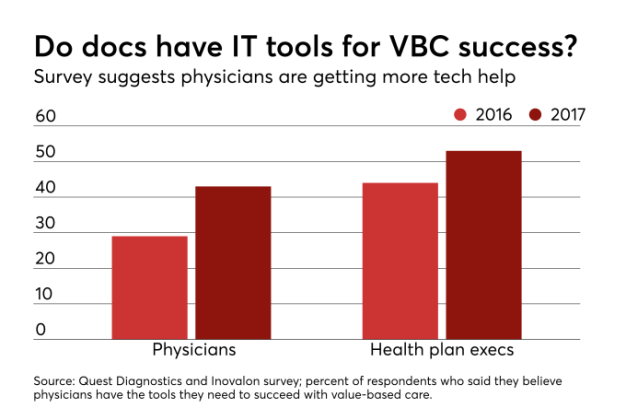
Results from innovation programs such as accountable care organizations, bundled payments and other ideas have not been as rosy as expected while bringing a number of attendant challenges. Those troubles are underscored by the findings from a recent survey conducted by Quest Diagnostics. In fact, the results are called “Stalled Progress on the Path to Value-Based Care,” which puts out the uncertain state without shying away from the perceived truth.
The survey reveals a slide among the viewpoints of physicians and, to a degree, health plan executives about the current state and viability of value-based care. On the whole, physicians are more skeptical. Some of the more interesting results are that a declining number of respondents believed the information necessary about patients to succeed with value-based care was in their hands.
Commentary frequently points to data as the lifeblood for being able to move ahead with value-based care. The dim view of data available in a physician’s electronic medical record helps provide color around falling assessment of whether sufficient data are available for success. Only 39 percent of responding physicians felt the EMR contained all the data needed for value-based care.
See Also: Shift to value-based care is slow, hampered by lack of IT, data
If so many physicians feel data are missing, where can that data be found? The cynical response would likely say in disparate systems that cannot talk to each other. While potentially overly cynical, the response is probably not without merit. The lack of interoperability, regardless of how it is defined, is not a myth within the system. While the technological means of remedying interoperability can probably be developed quickly or maybe even already exist, the will or incentive to put it into place is arguably missing.
Related to the data issue is the scope and applicability of quality measures. While this is an overused trope, if the quality measures in one value-based care plan are examined, then the reviewer likely only knows about one set of quality measures. Instead of developing and implementing a common set of quality measures, every value-based care program wants to come up with its own. This result can force providers into “focusing” on potentially hundreds of different quality measures that just sap time and energy from all involved.
Per the Quest survey, health plan executives more uniformly believe the measures can be helpful (80 percent) as opposed to a lower, though still majority, percentage of physicians (68 percent). While both areas of respondents leave a decent amount of room before all are on board, getting well over a majority for both suggests that quality measures are closer to hitting the mark than not.
Despite the potential usefulness of the measures being seen, both sides were very much aligned around the concept that measures are too complex. As noted above, it feels as though every value-based care program comes with its own measures. There could be five or more means of looking at blood pressure, diabetes management, smoking cessation or any other number of issues.
It is not clear why it is or should be so hard to come up with a common set of measures that can apply to any value-based care program. At some level, coming up with a proprietary program is more harmful than helpful.
One insight that can be inferred from the diverging views of physicians and health plan executives is that alignment between different aspects of the healthcare industry are still missing. Coming up with and putting into practice the means of getting the healthcare system into a more efficient, quality focused realm cannot be the work of any one segment of the industry. A fragmented approach will only lead to failure.
Could fraud and abuse regulations be a driver for the remaining gap between physicians, other providers, health plans and others in the industry? It is not a theory without merit. The fraud and abuse laws are arcane, convoluted and throw up a lot of barriers.
That is why the Centers for Medicare and Medicaid Services’ Request for Information concerning the Stark Law is important. The RFI squarely focuses on value-based care and how implementation and enforcement of the Stark Law can be changed to encourage value-based care. While exceptions arguably exist already that can be used to aid the creation of value-based care relationships, the law is rooted in a fee for service world and driven by concerns that may be alleviated and/or eliminated in a value-based care world.
Arguably CMS has already recognized that the Stark Law is incompatible with value-based care as a result of including numerous waivers with its different ACO models, bundled payment programs and other innovation models. The waivers, all self-certifying, provide fairly broad exemptions from the Stark Law for participants in order to more easily align workflows and divide shared savings. If the waivers were deemed necessary for the innovation models, it really begs the question of why the same waivers have not been expanded to encourage value-based car experimenting in other areas.
Leaving aside Medicare and other government-based programs, the private industry is not abandoning the value-based care world. Insurers such as UnitedHealth Group are, if anything, expanding such programs. Unlike Medicare, the private industry potentially has more freedom to adjust on the fly and account for issues such as those revealed by the Quest survey.
Ultimately, as has been noted before, the healthcare industry needed to change. The fee-for-service world could not remain rooted in place as costs were (and possibly still are) uncontrolled. The issue now is whether concerns about the ideas that have been put into place will be addressed and innovation allowed to occur, or will another misaligned system be allowed to pervade the industry.
Pope Francis has made no secret of his intention to radically reform the administrative structures of the Catholic church, which he regards as insular, imperious, and bureaucratic. He understands that in a hyper-kinetic world, inward-looking and self-obsessed leaders are a liability.
Last year, just before Christmas, the Pope addressed the leaders of the Roman Curia — the Cardinals and other officials who are charged with running the church’s byzantine network of administrative bodies. The Pope’s message to his colleagues was blunt.
Leaders are susceptible to an array of debilitating maladies, including arrogance, intolerance, myopia, and pettiness. When those diseases go untreated, the organization itself is enfeebled. To have a healthy church, we need healthy leaders.
Through the years, I’ve heard dozens of management experts enumerate the qualities of great leaders. Seldom, though, do they speak plainly about the “diseases” of leadership.
The Pope is more forthright. He understands that as human beings we have certain proclivities — not all of them noble. Nevertheless, leaders should be held to a high standard, since their scope of influence makes their ailments particularly infectious.
The Catholic Church is a bureaucracy: a hierarchy populated by good-hearted, but less-than-perfect souls. In that sense, it’s not much different than your organization. That’s why the Pope’s counsel is relevant to leaders everywhere.
With that in mind, I spent a couple of hours translating the Pope’s address into something a little closer to corporate-speak. (I don’t know if there’s a prohibition on paraphrasing Papal pronouncements, but since I’m not Catholic, I’m willing to take the risk.)
Herewith, then, the Pope (more or less):
____________________
The leadership team is called constantly to improve and to grow in rapport and wisdom, in order to carry out fully its mission. And yet, like any body, like any human body, it is also exposed to diseases, malfunctioning, infirmity. Here I would like to mention some of these “[leadership] diseases.” They are diseases and temptations which can dangerously weaken the effectiveness of any organization.
The disease of thinking we are immortal, immune, or downright indispensable, [and therefore] neglecting the need for regular check-ups. A leadership team which is not self-critical, which does not keep up with things, which does not seek to be more fit, is a sick body. A simple visit to the cemetery might help us see the names of many people who thought they were immortal, immune, and indispensable! It is the disease of those who turn into lords and masters, who think of themselves as above others and not at their service. It is the pathology of power and comes from a superiority complex, from a narcissism which passionately gazes at its own image and does not see the face of others, especially the weakest and those most in need. The antidote to this plague is humility; to say heartily, “I am merely a servant. I have only done what was my duty.”
Another disease is excessive busyness. It is found in those who immerse themselves in work and inevitably neglect to “rest a while.” Neglecting needed rest leads to stress and agitation. A time of rest, for those who have completed their work, is necessary, obligatory and should be taken seriously: by spending time with one’s family and respecting holidays as moments for recharging.
Then there is the disease of mental and [emotional] “petrification.” It is found in leaders who have a heart of stone, the “stiff-necked;” in those who in the course of time lose their interior serenity, alertness and daring, and hide under a pile of papers, turning into paper pushers and not men and women of compassion. It is dangerous to lose the human sensitivity that enables us to weep with those who weep and to rejoice with those who rejoice! Because as time goes on, our hearts grow hard and become incapable of loving all those around us. Being a humane leader means having the sentiments of humility and unselfishness, of detachment and generosity.
The disease of excessive planning and of functionalism. When a leader plans everything down to the last detail and believes that with perfect planning things will fall into place, he or she becomes an accountant or an office manager. Things need to be prepared well, but without ever falling into the temptation of trying to eliminate spontaneity and serendipity, which is always more flexible than any human planning. We contract this disease because it is easy and comfortable to settle in our own sedentary and unchanging ways.
The disease of poor coordination. Once leaders lose a sense of community among themselves, the body loses its harmonious functioning and its equilibrium; it then becomes an orchestra that produces noise: its members do not work together and lose the spirit of camaraderie and teamwork. When the foot says to the arm: ‘I don’t need you,’ or the hand says to the head, ‘I’m in charge,’ they create discomfort and parochialism.
There is also a sort of “leadership Alzheimer’s disease.” It consists in losing the memory of those who nurtured, mentored and supported us in our own journeys. We see this in those who have lost the memory of their encounters with the great leaders who inspired them; in those who are completely caught up in the present moment, in their passions, whims and obsessions; in those who build walls and routines around themselves, and thus become more and more the slaves of idols carved by their own hands.
The disease of rivalry and vainglory. When appearances, our perks, and our titles become the primary object in life, we forget our fundamental duty as leaders—to “do nothing from selfishness or conceit but in humility count others better than ourselves.” [As leaders, we must] look not only to [our] own interests, but also to the interests of others.
The disease of existential schizophrenia. This is the disease of those who live a double life, the fruit of that hypocrisy typical of the mediocre and of a progressive emotional emptiness which no [accomplishment or] title can fill. It is a disease which often strikes those who are no longer directly in touch with customers and “ordinary” employees, and restrict themselves to bureaucratic matters, thus losing contact with reality, with concrete people.
The disease of gossiping, grumbling, and back-biting. This is a grave illness which begins simply, perhaps even in small talk, and takes over a person, making him become a “sower of weeds” and in many cases, a cold-blooded killer of the good name of colleagues. It is the disease of cowardly persons who lack the courage to speak out directly, but instead speak behind other people’s backs. Let us be on our guard against the terrorism of gossip!
The disease of idolizing superiors. This is the disease of those who court their superiors in the hope of gaining their favor. They are victims of careerism and opportunism; they honor persons [rather than the larger mission of the organization]. They think only of what they can get and not of what they should give; small-minded persons, unhappy and inspired only by their own lethal selfishness. Superiors themselves can be affected by this disease, when they try to obtain the submission, loyalty and psychological dependency of their subordinates, but the end result is unhealthy complicity.
The disease of indifference to others. This is where each leader thinks only of himself or herself, and loses the sincerity and warmth of [genuine] human relationships. This can happen in many ways: When the most knowledgeable person does not put that knowledge at the service of less knowledgeable colleagues, when you learn something and then keep it to yourself rather than sharing it in a helpful way with others; when out of jealousy or deceit you take joy in seeing others fall instead of helping them up and encouraging them.
The disease of a downcast face. You see this disease in those glum and dour persons who think that to be serious you have to put on a face of melancholy and severity, and treat others—especially those we consider our inferiors—with rigor, brusqueness and arrogance. In fact, a show of severity and sterile pessimism are frequently symptoms of fear and insecurity. A leader must make an effort to be courteous, serene, enthusiastic and joyful, a person who transmits joy everywhere he goes. A happy heart radiates an infectious joy: it is immediately evident! So a leader should never lose that joyful, humorous and even self-deprecating spirit which makes people amiable even in difficult situations. How beneficial is a good dose of humor!
The disease of hoarding. This occurs when a leader tries to fill an existential void in his or her heart by accumulating material goods, not out of need but only in order to feel secure. The fact is that we are not able to bring material goods with us when we leave this life, since “the winding sheet does not have pockets” and all our treasures will never be able to fill that void; instead, they will only make it deeper and more demanding. Accumulating goods only burdens and inexorably slows down the journey!
The disease of closed circles, where belonging to a clique becomes more powerful than our shared identity. This disease too always begins with good intentions, but with the passing of time it enslaves its members and becomes a cancer which threatens the harmony of the organization and causes immense evil, especially to those we treat as outsiders. “Friendly fire” from our fellow soldiers, is the most insidious danger. It is the evil which strikes from within. As it says in the bible, “Every kingdom divided against itself is laid waste.”
Lastly: the disease of extravagance and self-exhibition. This happens when a leader turns his or her service into power, and uses that power for material gain, or to acquire even greater power. This is the disease of persons who insatiably try to accumulate power and to this end are ready to slander, defame and discredit others; who put themselves on display to show that they are more capable than others. This disease does great harm because it leads people to justify the use of any means whatsoever to attain their goal, often in the name of justice and transparency! Here I remember a leader who used to call journalists to tell and invent private and confidential matters involving his colleagues. The only thing he was concerned about was being able to see himself on the front page, since this made him feel powerful and glamorous, while causing great harm to others and to the organization.
Friends, these diseases are a danger for every leader and every organization, and they can strike at the individual and the community levels.
____________________
So, are you a healthy leader? Use the Pope’s inventory of leadership maladies to find out. Ask yourself, on a scale of 1 to 5, to what extent do I . . .
Feel superior to those who work for me?
Demonstrate an imbalance between work and other areas of life?
Substitute formality for true human intimacy?
Rely too much on plans and not enough on intuition and improvisation?
Spend too little time breaking silos and building bridges?
Fail to regularly acknowledge the debt I owe to my mentors and to others?
Take too much satisfaction in my perks and privileges?
Isolate myself from customers and first-level employees?
Denigrate the motives and accomplishments of others?
Exhibit or encourage undue deference and servility
Put my own success ahead of the success of others?
Fail to cultivate a fun and joy-filled work environment?
Exhibit selfishness when it comes to sharing rewards and praise?
Encourage parochialism rather than community?
Behave in ways that seem egocentric to those around me?
As in all health matters, it’s good to get a second or third opinion. Ask your colleagues to score you on the same fifteen items. Don’t be surprised if they say, “Gee boss, you’re not looking too good today.” Like a battery of medical tests, these questions can help you zero in on opportunities to prevent disease and improve your health. A Papal leadership assessment may seem like a bit of a stretch. But remember: the responsibilities you hold as a leader, and the influence you have over others’ lives, can be profound. Why not turn to the Pope — a spiritual leader of leaders — for wisdom and advice?
Gary Hamel is visiting professor at London Business School and cofounder of The Management Innovation Exchange. His latest book is “What Matters Now.”
In an opinion piece for the Sunday Times in August 2018, Jeremy Fleming underlines the importance of partnerships in the new digital age.
News article – 12 August 2018
Director GCHQ, Jeremy Fleming, writes about the unparalleled opportunities and challenges we face as the world becomes ever more digitally connected. With the globalisation of technology, he explains how GCHQ will continue to work with businesses, technology companies, academia, and privacy groups, to protect the public from real-world and online harm.
We have entered a new technological age, one that will fundamentally change the way we live, work and interact with each other. This new digital landscape will transform lives and economies as data analysis, artificial intelligence, 5G, the internet of things, quantum computing and many other technologies still being developed permeate all areas of human endeavor.
These changes will bring huge benefits to us all. They will transform healthcare, create smart, energy-efficient cities, make work lives more productive and revolutionize the relationship between business and the consumer. But they also bring risks that, if unchecked, could make us more vulnerable to terrorists, hostile states and serious criminals.
Getting the balance right requires new partnerships and different ways of working at a global level.
The key to securing the benefits of this new age lies in the way in which we secure personal information and new technologies from those seeking to do us harm. In the past we have often seen security bolted on to technology as new risks emerge. For an environment where the cycle of development to deployment is accelerating and where our dependence on overseas technologies is increasing, this approach no longer works.
New systems – and their supply chains – need security built into the earliest stages of design if we are to protect liberties, ensure public confidence and counter threats to internet freedom.
GCHQ has always played a prominent role in this space. Now it is the mission of the National Cyber Security Centre (NCSC) – part of GCHQ – to make the UK the safest place to live and do business online.
This is an enormous challenge, but less than two years after its formation we can already see how its leadership role is making a difference to the cyber-health of the nation. Since the NCSC’s inception we have been critical in responding to and reducing the harm from more than 1,000 cyber-attacks against the UK.
It is also increasingly clear that as the world becomes ever-more networked, we need to work even harder with businesses, technology companies, academia and privacy groups to protect the public from real-world and online harm.
We need honest, mature conversations about the impact that new technologies could have on society. This needs to happen while systems are being developed, not afterwards. And in doing so we must ensure that we protect our right to privacy and maximise the tremendous upsides inherent in the digital revolution.
This isn’t easy. However, I can see it taking shape in some key areas. There is already an important public debate about the exceptional circumstances when law enforcement and the intelligence services should access encrypted communications – something we know has potential technical solutions in most cases.
We believe some principles allowing industry and governments to demonstrate responsible access that protects privacy are within reach.
These do not require unfettered access for governments through so-called “back door” or global “skeleton key” schemes. But they do require public debate and close, open co-operation and agreement with technology companies. And when these solutions exist, they also require modern legislation and strong oversight to maintain public confidence.
We now have that in the UK where the Investigatory Powers Act is world leading in the oversight of exceptional access requests, with legal authorisations jointly signed by a secretary of state and an independent judge.
For this kind of approach to succeed we must work more closely with partners – not just here in the UK, but across Europe and the globe. We and our allies all face the same challenges.
The globalisation of technology is here and we need to learn to deal with it. Critical technologies – for example, in 5G – are increasingly likely to come from China. The British government recently published its national security and investment white paper on foreign direct investment into the UK and we are looking at how we can better manage supply to our critical national infrastructure (CNI).
We must ensure that processes represent industry best practice so as to avoid real risk to the UK’s CNI. We need to consider early, robust and fair solutions to the global challenge of balancing investment, trade and security.
Just as our adversaries are not constrained by international boundaries, we must make sure that our legislative and technology arrangements are able to keep pace. The ability for countries with strong privacy protection such as the UK to request a user’s data held by US communication companies on serious criminal and terrorism grounds – the Cloud Act – is an excellent example of what is possible.
This is just one step towards agile security. As a nation, there is still much to be done to respond to the challenges to come. Stepping up to that responsibility, GCHQ will continue to build on our world-class understanding of technology to inform government policy and protect the UK. And we will continue to harness the nation’s full diversity of thought and talent and demonstrate the kind of ingenuity that has defined GCHQ and our people for almost 100 years.
By working with partners – both here and abroad – we can be prepared for the unparalleled opportunities that the new data-driven world will bring.
Health IT stakeholder groups are frustrated with what they see as lack of progress from the government in combating the practice of information blocking, according to a letter sent to the Office of the National Coordinator for Health IT (ONC).
One of the promises of the 21st Century Cures Act, which was passed by Congress at the end of 2016, was that it mandated the creation of regulations that prohibit providers and health IT developers from engaging in information blocking. Information blocking is one of the biggest hurdles to the free flow of health data from one organization to another—known as interoperability. According to Health IT Now, which is made up of 14 health IT stakeholder groups, the Cures Act required ONC to issue regulations halting information blocking, as well as create a standardized process where members of the public could report instances where health IT products are not interoperable or where other activities actively hamper information exchange.
“As the administration proposes and implements new rules related to open APIs and interoperability in Medicare’s payment rules for hospitals and doctors, the lack of clear rules of the road needlessly create uncertainty for vendors and providers alike,” they wrote.
The letter, which is dated August 6, 2018, notes that it’s been over 600 days since the law’s passage. “The administration has had 601 days to draft and publish clear information blocking regulations. We understand the nuance required, but feel that it is past time for a proposal to be made.” In a speech at ONC’s Interoperability Forum this week, ONC chief Don Rucker, MD, said that the information blocking regulations are a “work in progress,” according to Politico. Rucker said the timetable for releasing regulations has been pushed back to September.
ONC defines information blocking as “an act or a course of conduct that interferes with the ability to exchange or use electronic health information where permitted/authorized.” Examples include “implementing fees that make data exchange cost prohibitive, or technology designed or implemented in non-standard ways that inhibit the exchange of information.”
The 21st Century Cures Act provides a number of ways for the industry to challenge such practices, such as identifying reasonable and necessary activities that do not constitute information blocking, and allowing the Department of Health and Human Services Office of the Inspector General (OIG) to investigate credible claims of information blocking.
Health IT Now also addressed its letter to the OIG. To read it, click here.
Rucker previewed ONC’s actions on information blocking in a blog post for the journal Health Affairs.
 Report at a Glance
Report at a Glance

 Then there was the
Then there was the